
New Jersey
Health Information Technology
Environmental Scan
Final Report
September 2017

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
I
Table of Contents
Table of Contents i
Table of Figures iii
Executive Summary 1
New Jersey Innovation Institute 2
New Jersey “As-Is” Health Information Technology Landscape 3
Population 3
Providers 3
Hospitals 5
Health Information Technology and Electronic Health Records Adoption Survey 6
Methodology: Survey Design, Data Collection, and Analysis 6
NJ Environmental Scan Survey Respondent Population Demographics 7
Insurance Profile 11
Use of Electronic Health Records 12
Satisfaction with and Capabilities of EHR System 14
Privacy and Security Risk Assessment 15
Barriers to Using an EHR 16
Prevalence of Other Health Information Technologies 16
Health Information Exchange 17
Medicare/Medicaid Meaningful Use 18
Electronic Health Data Capabilities 20
Sharing Patient or Client Health Information 21
Electronic Data Sharing 21
Discharge Summaries 22
Preferences for Future Electronic Data Sharing 23
Medical Home Model and Alternative Payment Model 23
Demographics 23
Providers affiliated with Community Health Centers (Federally Qualified Health Centers (FQHC)) 24
Broadband Internet Access 24
Quick Statistics 24
Broadband Access 24
Federally Qualified Health Centers (FQHCs) 25

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
II
Health Information Exchange Presence in New Jersey 26
NJ HIE Core Services 28
NJ HIE Advanced Services 28
NJ HIE Value Services 29
New Jersey Health Information Exchange Organizations 30
State Activities to Facilitate HIE and EHR Adoption 31
HIO/HIE Activities across State Borders 32
HIO/HIE Interoperability 32
Conclusion: Key Findings 33
EHR Adoption 33
Health Information Exchange 33
Health Information Technology 34
Broadband Coverage 34
Education 34
NJ’s HIT Landscape to Continue to Evolve by Leveraging HIT Capabilities 34
Appendix A: List of Abbreviations 35
Appendix B: HIT Coverage on Geographic Maps of New Jersey 37
Appendix C: Population Data of New Jersey 40
A Profile of New Jersey’s Physicians 42
Revision History 43
References 44

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
III
Table of Figures
Figure 1. Percent of NJ Physicians that Adopted Any, Basic, and Certified EHRs based on the 2015
CDC/NCHS National Electronic Health Records Survey.
Figure 2. Percent of NJ Physicians that Adopted Certified EHRs by Physician Specialty based on the 2015
CDC/NCHS National Electronic Health Records Survey.
Figure 3. Percent of NJ Physicians that Adopted Certified EHRs by Physician Specialty based on the 2015
CDC/NCHS National Electronic Health Records Survey.
Figure 4. Percent of NJ Hospitals the electronically share Data based on the 2015 CDC/NCHS National
Electronic Health Records Survey.
Figure 5. 2017 NJ Health Information Technology Survey Respondents by Provider Type.
Figure 6. NJ 2017 Health Information Technology Survey Specialty breakdown, with available specialty
data from physicians and nurse practitioners.
Figure 7. Provider Affiliations with Healthcare Institutions in the NJ 2017 Health Information Technology
Survey.
Figure 8: Insurance Acceptance by Provider Type in the NJ 2017 Health Information Technology Survey.
Figure 9. Specialists accepting Medicaid/CHIP in the NJ 2017 Health Information Technology Survey.
Figure 10. EHR Use by Provider in the NJ 2017 Health Information Technology Survey.
Figure 11. Hospital-based Providers’ EHR Use of Electronic, Mixed (Electronic and Paper), or None in the
NJ 2017 Health Information Technology Survey.
Figure 12. Provider Satisfaction with their Electronic Health Record systems in the NJ 2017 Health
Information Technology Survey.
Figure 13. ONC Certification Rates for Providers’ EHRs according to the NJ 2017 Health Information
Technology Survey.
Figure 14. Risk Assessments Completion Rate according to the NJ 2017 Health Information Technology
Survey.
Figure 15. Percentage of Barriers Providers Reported For Not Using an EHR in the NJ 2017 Health
Information Technology Survey.
Figure 16. Percentage of HIE Connected Providers Among Survey Respondents
Figure 17. HIE Satisfaction Rates Among Survey Respondents.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
IV
Figure 18. Percentage of Provider Reasons for Not Participating in a Health Information Exchange in the
NJ 2017 Health Information Technology Survey.
Figure 19. Percentage of Meaningful Use EHR Incentive Participants Among Survey Respondents.
Figure 20. Percentage of Meaningful Use Stage 3 Incentive Payment Status Among Survey Respondents.
Figure 21. EHR Capabilities in the NJ 2017 Health Information Technology Survey.
Figure 22. Online Capabilities for Patients in the NJ 2017 Health Information Technology Survey.
Figure 23. Types of Information and Data Sharing Rates Among Providers who Share Electronic
Information in the NJ 2017 Health Information Technology Survey.
Figure 24. Access to Broadband Internet in NJ.
Figure 25. Broadband Speed Availability.
Figure 26. Number of Community Health Center such as Federally Qualified Health Center (FQHC),
federally-funded clinics, “look-alike” clinics, or satellite locations distributed by County in NJ.
Figures 27a-d. Hospitals Connected to the HIE; Users connected and using HIE Services; Unique patients
contained in system; Patient portal users.
Figure 28. Jersey Health Connect Service Catalog and NJHIN Comparison.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
1
Executive Summary
The New Jersey Department of Human Services (DHS), Division of Medical Assistance and Health Services
(DMAHS), in the process of updating the State Medicaid Health Information Technology Plan (SMHP) conducted
a Health Information Technology (HIT) Environmental Scan. The purpose of the HIT Environmental Scan is to
provide the State with an understanding of the current healthcare technology landscape which will assist in
developing the strategy and future direction of the SMHP.
The SMHP provides State Medicaid Agencies (SMAs) and the Centers for Medicare and Medicaid Services (CMS)
with a common understanding of the activities the SMA will be engaged in over the next 5 years relative to
implementing Section 4201 Medicaid provisions of the American Recovery and Reinvestment Act (ARRA).
Between 2016 and 2017, New Jersey Innovations Institute (NJII) Healthcare Delivery Systems iLab, a non-profit
corporation of the New Jersey Institute of Technology, was tasked with conducting the HIT Environmental Scan
in New Jersey based on an agreement with DMAHS and as approved by CMS.
The New Jersey Department of Health (NJDOH) selected NJII as the State Designated Entity (SDE) to establish the
New Jersey Health Information Network (NJHIN), which is administered by the NJDOH. The NJHIN is also
supported by the State Health IT Coordinator. Toward fulfilling the main goal of statewide exchange, the NJHIN
team is working to connect major Health Information Exchange Organizations (HIEs/HIOs), health
systems/hospitals, and other healthcare organizations in New Jersey.
As agreed upon with DMAHS, NJII collected and analyzed information on data items listed below.
1. Current New Jersey population
2. Current provider numbers
3. Current state of Health Information Exchanges (HIE/HIO) in New Jersey
3.1 Health Information Exchange future strategy
3.2 The New Jersey Health Information Network
3.3 Current status/State activities to facilitate HIE
3.4 Interoperability with public health registries
3.5 Sustainability strategy
4. Health Information Exchange Adoption
4.1 Eligible Professional (EP) and Eligible Hospital (EH)
5. Electronic Health Record adoption
5.1 Eligible Professional and Eligible Hospital
6. Meaningful Use adoption
6.1 Eligible Professional and Eligible Hospital
7. Broadband internet access
8. Federally Qualified Health Centers (FQHC)
8.1 Number and geographic locations
8.2 Electronic Health Record (EHR) adoption
8.3 Meaningful Use (MU) adoption
8.4 Health Information Exchange Adoption
9. Other Federal and State grants relevant to Health Information Technology

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
2
New Jersey Innovation Institute
The New Jersey Innovation Institute (NJII) is a New Jersey Institute of Technology (NJIT) non-profit corporation
that applies the intellectual and technological resources of the state’s science and technology university to
challenges identified by industry partners. Through its Innovation Labs (iLabs), NJII brings NJIT expertise to key
economic sectors, including healthcare delivery systems, bio-pharmaceutical production, civil infrastructure,
defense and homeland security, and financial services.
The NJII Healthcare Delivery Systems iLab was formerly known as the New Jersey-Health Information
Technology Extension Center (NJ-HITEC), the Regional Extension Center (REC) for Meaningful Use (MU) in New
Jersey. NJ-HITEC had been established in 2010 as an unincorporated center of program activity at NJIT through a
$23 million grant from the federal Department of Health and Human Services’ Office of the National Coordinator
for Health Information Technology (ONC) as part of the 2009 American Recovery and Reinvestment Act (ARRA)
law.
NJII continues to meet the needs of NJ-HITEC’s provider members, consisting of 9,600 primary care providers
(PCPs) and specialists, throughout New Jersey by supporting hospitals and providers in the electronic exchange
of medical records as they endeavor to continue attestation to Meaningful Use. NJII and NJ-HITEC have more
than seven years of experience working with providers and hospitals to navigate through the complexities of
health information exchange in New Jersey. Over the past seven years, NJII has helped member providers
receive more than $100 million in incentive payments. The currently ongoing Medicaid Provider Program (MPP)
grant was awarded to NJII/NJ-HITEC based on the success of the REC program. As of the end of June 2017, the
NJII MPP have assisted in the successful attestation of 594 Medicaid providers and 1,638 MPP provider
members have received a Medicaid MU payment as of July 2017.
Committed to improving healthcare through innovative programs and services, NJII Healthcare Delivery Systems
iLab’s Garden Practice Transformation Network (PTN) program is moving more than 10,000 physicians from fee-
for-service to value-based care as part of the Centers for Medicare & Medicaid Services (CMS) Transforming
Clinical Practices Initiative. Through the program, NJII will save more than $135 million in healthcare costs and
improve the lives of more than 500,000 patients with chronic illnesses.
The iLab is also driving the healthcare technological revolution in our State through the New Jersey Health
Information Network (NJHIN), a shared services platform developed by the New Jersey Department of Health
(NJDOH) and powered by NJII that is enabling statewide data sharing by connecting health information exchange
organizations (HIE/HIO), hospitals, and clinicians together though admission, discharge, and transfer (ADT)
alerts, immunization data, and a Master Person Index (MPI) that uniquely identifies patients across the
healthcare continuum. Additionally, NJHIN's Use Cases are empowering more than 500 providers and over 20
Long Term and Post-Acute Care (LTPAC) facilities to have access to State public health registries and other
healthcare stakeholders' data sharing sources to drive improvements in clinical outcomes and population health.
The iLab also partners with physicians to help them report on Federal and State administered quality
improvement programs, including the Merit-based Incentive Payment Program (formerly Medicare EHR
Incentive Program and Physician Quality Reporting System), the Delivery System Reform Incentive Payment
Program, and Accountable Care Organizations. In 2016, NJII’s member hospitals received more than $47.6
million in incentive payments.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
3
New Jersey “As-Is” Health Information Technology Landscape
Population
NJ is ranked number 1 in population density among the 50 States, with a population of 8,944,469 across 21
counties.
Providers
The population is served by a total of 25,930 active physicians. There are 8,569 primary care providers (PCP)
providing a ratio of 1 PCP for every 1,104 state residents.
Total Active Physicians:
25,930
Primary Care Physicians:
8,569
Total Residents:
2,875
Total Female Physicians:
9,045
Total Medical or Osteopathic Students:
2,177
With the goal of providing the State of New Jersey with an understanding of the current healthcare technology
landscape, the 2017 Health Information Technology (HIT) Environmental Scan was primarily based on the
questions contained in the 2014 National Electronic Health Records Survey along with questions based on new
New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
4
HIT trends such as the adoption and use of Health Information Exchange and other technologies. We also
evaluated data contained in our NJII/NJ-HITEC databases and other sources to produce this report.
Since key objectives of the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009
included measuring the adoption and meaningful use of electronic health records (EHRs), this report contains a
review of New Jersey’s HIT adoption landscape. Among non-federal acute care hospitals in New Jersey, adoption
of basic EHR systems has increased from 16% to 75% between 2008 and 2015
i
. Moreover, 95% of New Jersey’s
Eligible Hospitals (EH) adopted and demonstrated meaningful use of certified health IT (CEHRT) through the
Centers Medicare and Medicaid Services (CMS) EHR Incentive Programs
ii
.
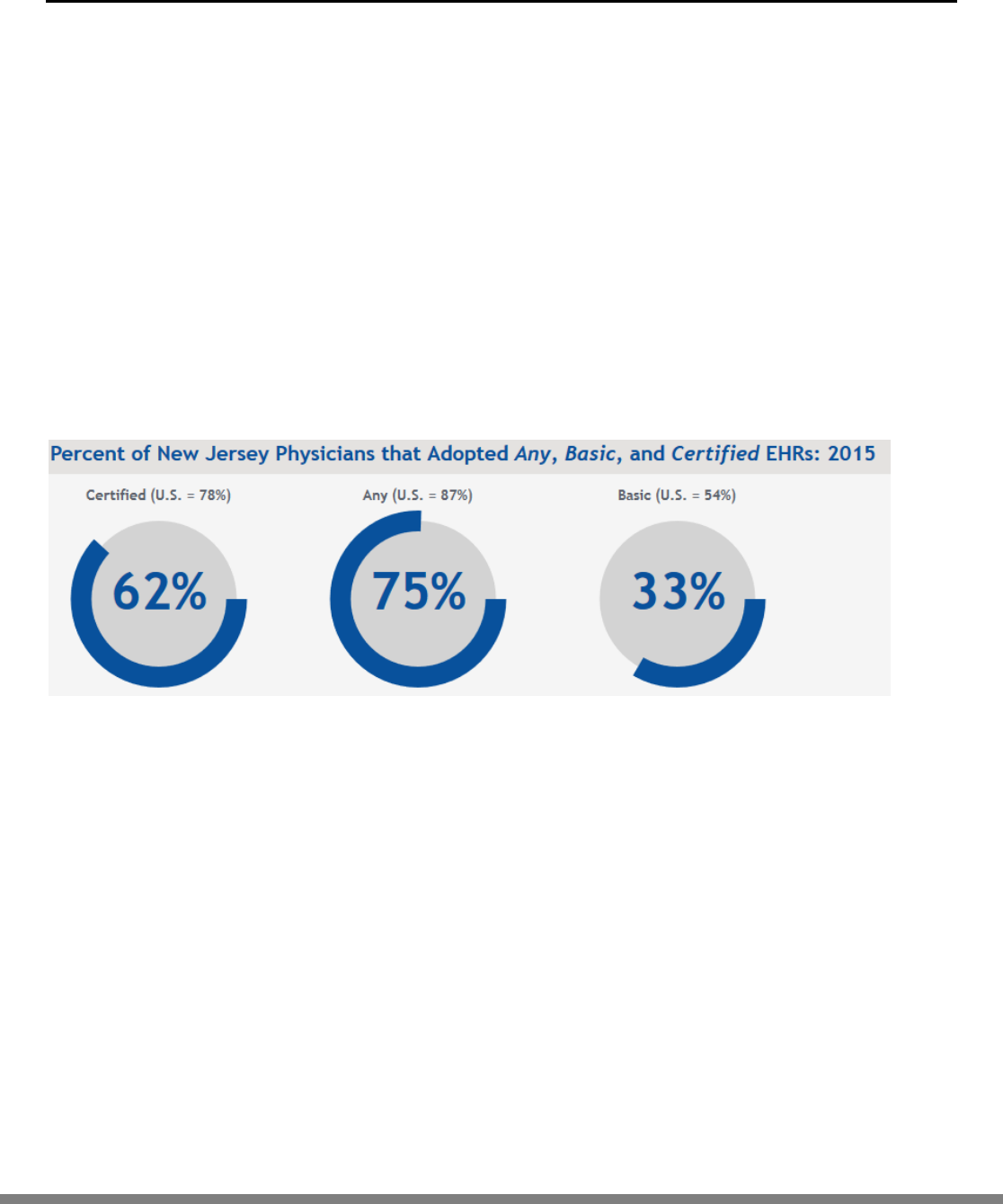
Although the State have seen an increase in EHR adoption rates since the advent of the EHR Incentive Programs,
the Centers for Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS) National
Electronic Health Records Survey in 2015 revealed that New Jersey’s office-based physician adoption of either
“Any” (electronic medical record excluding billing record systems), “Basic” (a system with the following
capabilities: patient demographics, clinician notes, patient problem lists, patient medication lists, prescription
orders, viewing imaging results, and viewing laboratory results), or “Certified” (any EHR that met Meaningful
Use criteria) is still somewhat lower than national adoption rates
iii
.
Figure 1. Percent of NJ Physicians that Adopted Any, Basic, and Certified EHRs based on the 2015 CDC/NCHS
National Electronic Health Records Survey.
Further comparisons between the adoption of certified EHRs by primary care and specialist physicians (“a
primary care physician specializes in one of the following areas: adolescent medicine, pediatrics, family practice,
general practice, geriatrics, internal medicine, obstetrics, or gynecology. A specialist is a non-primary care
medical or surgical physician specialist”
iv
) revealed the following:

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
5
Figure 2. Percent of NJ Physicians that Adopted Certified EHRs by Physician Specialty based on the 2015
CDC/NCHS National Electronic Health Records Survey.
Hospitals
New Jersey currently has 75 Hospitals comprising of 20,589 Staffed beds. New Jersey hospitals reflect similar
levels to the national averages on adoption of a Certified Electronic Health Record.
Figure 3. Percent of NJ Physicians that Adopted Certified EHRs by Physician Specialty based on the 2015
CDC/NCHS National Electronic Health Records Survey.
Sharing of data from outside health providers demonstrates above average against the national landscape
however there is also still room to improve. Additionally, the data does not show if the data is consumed,
integrated in clinical workflows, or used in patient care.
Figure 4. Percent of NJ Hospitals the electronically share Data based on the 2015 CDC/NCHS National Electronic
Health Records Survey.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
6
Health Information Technology and Electronic Health Records Adoption Survey
Methodology: Survey Design, Data Collection, and Analysis
In collaboration with Rutgers University’s Eagleton Center for Public Interest Polling, the research
application to conduct this Environmental Scan survey was submitted to the Rutgers University Institutional
Review Board (IRB) in January 2017 and approved in February 2017. The 2017 New Jersey Health
Information Technology Survey was fielded between March 15, 2017 and May 31, 2017 and during which
responses were collected. The survey was sent to all physicians (Medical Doctors and Doctors of
Osteopathic Medicine), dentists (Doctors of Dental Surgery and Doctor of Medicine in Dentistry),
optometrists, and advance practice nurses (Nurse Practitioners) licensed to practice in the State of New
Jersey who had contact addresses on their license listed in the State of New Jersey.
Collectively, these four groups are termed “providers.” Contact information for providers was obtained
from proprietary and State databases. Providers with email addresses were emailed the survey. Those
without email addresses were sent notices through fax numbers or via postcard, if a fax number was not
available. Each provider was given a unique code with which to access the survey, in order to prevent
duplicate responses.
Though all correspondence was addressed to the provider, either the provider or a member of their office
staff (such as an office manager) was eligible to complete the survey. For analytical purposes, unless
otherwise specified, we placed respondents identifying as office staff completing the survey on behalf of
the provider in the same category as their respective provider. Provider specialties, when available, were
recorded for physicians and nurse practitioners responding to at least one question on the survey.
Across all four provider groups, a total of 22,917 received the survey via email, 1,767 by fax, and 3,197 via
postcard, for a total of 27,881 unique contacted providers. All respondents contacted via email were
contacted regarding participation 3-5 times between March 15, 2017 and April 27, 2017. Faxes with an
invitation to take the survey were sent on April 5, 2017, and postcards were sent on April 10, 2017. An
additional batch of postcards was sent on May 25, 2017 to both postcard and fax recipients who had not
yet responded. During our outreach efforts, the majority of the contacts had email addresses; those
individuals were contacted by email only. We ensured that no provider was listed twice on any list for
method of contact, which means that a unique amount of providers were contacted by email, fax, and
postcard and that they each received a unique survey link.
Environmental Scan Survey Outreach Numbers for New Jersey Providers
Provider Type
Email
Fax
Postcard
Total per Type
Physicians
15687
1644
350
17681
Dentists
1214
123
362
1699
Optometrists
821
0
622
1443
Nurse Practitioners
5195
0
1863
7058
Total per Outreach
22917
1767
3197
27881

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
7
The survey, largely adapted from the long form of the Centers for Disease Control and Prevention (CDC)
National Center for Health Statistics (NCHS)’s 2014 National Electronic Health Records Survey (affiliated
with the National Ambulatory Medical Care Survey), contained questions on the following topics:
Use of Electronic Health Records (EHR) and Health Information Technology (HIT)
Adoption of Health Information Exchanges (HIE)
Adoption of Meaningful Use (MU) criteria
Insurance coverage
Access to high speed internet
Features of EHR
Perceived benefits of EHR and HIT
Barriers to EHR and HIT adoption
Results are reported as all responses with only valid responses (i.e. without missing values); thus, the number of
total responses on each question may differ from the next. All data reported are unweighted frequencies.
Descriptive statistics are used to describe the data. Percentages may not add up to 100 percent due to rounding,
or because respondents were allowed to select multiple response options.
Respondents replied to survey questions in the context of their “reporting location” – the setting in which they
saw the most patients or clients in a normal week. A “normal week” was defined as a week with a normal
caseload, with no holidays, vacations, or conferences.
NJ Environmental Scan Survey Respondent Population Demographics
A total of 1,384 respondents began the NJ Health Information Technology Survey during the 2017 response
collection period. Of these, 957 answered the question regarding the presence of an electronic health record
(EHR) system in their practice, and 546 completed the entire survey. The overall response rate for the survey of
completed cases was 2.4 percent for completed cases.
In an effort to amass greater statistical confidence in results, studies of elite populations frequently incentivize
respondents in order to boost response rates.
v
Our study faced a challenge with the response rate due to the
inability to incentivize participation. While methods to mitigate the bias introduced by survey nonresponse in
probability surveys are well established, these methods can be applied only to surveys in which a sample of
respondents are chosen at random from a population. In these methods, information about the population is
available, and statistics are reported with confidence intervals as a way of identifying the degree of uncertainty
(potential bias) of the results.
In our survey, however, we conducted census of all physicians, dentists, optometrists, and nurse practitioners in
the state of New Jersey, in which all participants of the population were invited to participate. Unlike those for
probability surveys, methods for correcting and reporting bias in nonprobability surveys are still up for debate.
We used the method for estimating the maximum absolute value of the bias in web surveys developed by
Bethlehem (2010)
vi
[Equation 14] to account for self‐selection into participating in the survey. We calculated
that the maximum absolute bias in the survey as 5.69, which suggests that the results should be interpreted
with caution.
Of the total 1326 providers responding to the question regarding provider type, 48 percent were physicians (or
office staffers replying on behalf of physicians), 10 percent were dentists, 8 percent were optometrists, and 34
percent were nurse practitioners.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
8
Figure 5. 2017 NJ Health Information Technology Survey Respondents by Provider Type.
Responding physicians and nurse practitioners represented an array of medical specialties in the 2017 NJ Health
Information Technology Survey. The specialties with the largest representation in the survey were Internal
Medicine (16 percent), Family Medicine (16 percent), and Pediatrics (13 percent).

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
9
Figure 6. NJ 2017 Health Information Technology Survey Specialty breakdown, with available specialty data from
physicians and nurse practitioners.
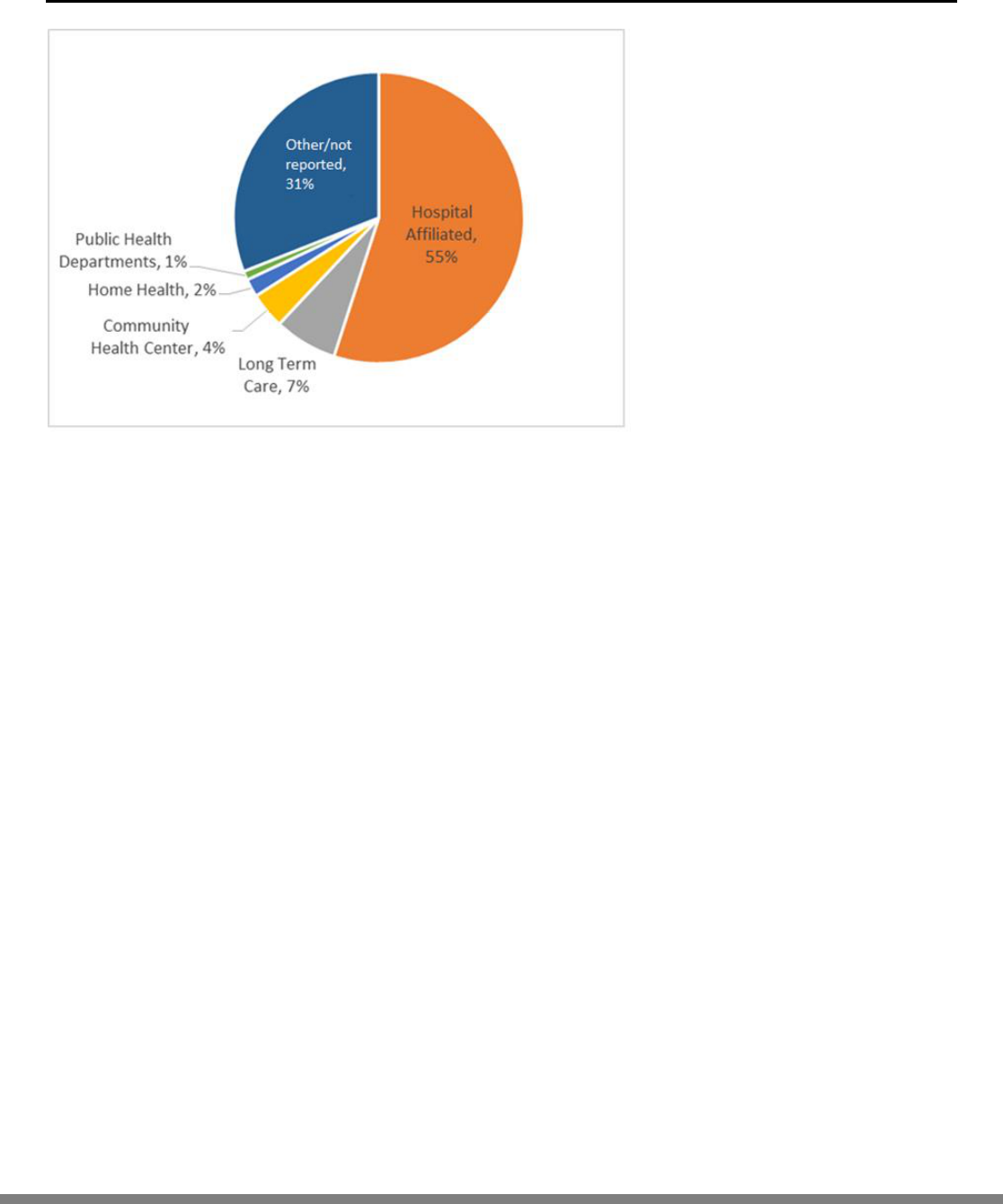
The majority of responding providers reported working in or being currently affiliated with a hospital (55
percent), Seven percent were affiliated with a long-term care facility, and only 4 percent reported having an
affiliation with a Community Health Center (e.g. a Federally Qualified Health Center (FQHC), federally-funded
clinics, or “look-alike” clinics.) Two (2) percent were affiliated with home health agencies and community mental
health centers, respectively, and 1 percent worked or were affiliated with public health departments or a
substance use disorder treatment center. Thirty-eight percent reported not working in any of the
aforementioned facilities.
The majority of providers reported seeing patients in a group or solo practice setting: Of the 47 total responding
office staff members, nearly all (98 percent) reported that the provider for which they worked was in group or
solo practice. Sixty-six percent of providers reported the same. Thirty-five percent of providers reported seeing
patients in hospital inpatient settings and 22 percent in hospital emergency departments or hospital outpatient
settings. Other providers saw patients in freestanding clinics/urgent care centers (8 percent) or in a faculty
practice setting (7 percent). Four (4) percent saw patients in a community health center, and 3 percent in a clinic
not affiliated with the federal government. The majority of providers (66 percent) saw patients or clients at only
one office location in a normal week, with the median number of locations being reported as 1 [interquartile
range: 1].
New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
10
Figure 7. Provider Affiliations with Healthcare Institutions in the NJ 2017 Health Information Technology Survey.
Providers (including their office staff) reported seeing patients in various settings during a normal week (defined
as a week with a normal caseload, with no holidays, vacations, or conferences). The majority were in private
practice (in a solo or group setting, 51 percent), followed by hospital inpatient settings (18 percent), hospital
emergency departments or hospital outpatient departments (14 percent), faculty practices (7 percent), and
freestanding clinic or urgent care centers (6 percent). Only 2 percent of providers had a reporting location of a
community health center (e.g. a Federally Qualified Health Center (FQHC), federally-funded clinics, or “look-
alike” clinics), and 1 percent were mental health centers, non-federal government clinics (e.g., state, county,
city, maternal and child health, etc.), or health maintenance organizations, or other prepaid practice (e.g.
Horizon HealthCare Plan of New Jersey). These locations are referred to as the “reporting location” for the
respondent.
Accordingly, 54 percent of providers stated that their reporting location (the setting in which they saw the most
patients per week) was owned by a physician or provider group, 81 percent of which were single group
practices; another 12 percent indicated a reporting location of an academic medical center. A median number of
the providers employed in the reporting location was 3 [IQR: 6]. All providers except nurse practitioners and
their staff estimated the median number of mid-level providers (i.e. nurse practitioners, physician assistants,
and nurse midwives) at their reporting location as 1 [IQR: 6].

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
11
Insurance Profile
Respondents accepted a variety of insurance plans, which varied by provider type. Nearly all (97 percent) of
providers reported accepting new patients at the time of the survey, and most reported accepting non-capitated
private insurance (90 percent) and self-payment (94 percent) for services. Across all provider types, 82 percent
accepted Medicare and 63 percent Medicaid as payment for services. Sixty-two (62) percent accepted insurance
capitated payment, and 55 percent accepted workers’ compensation. Within provider types, 86 percent of
physicians reported accepting Medicare, as did 23 percent of dentists, 90 percent of optometrists, and 87
percent of nurse practitioners. However, providers were less likely to accept Medicaid/CHIP (including Medicaid
Managed Care): 64 percent of physicians reported accepting Medicaid, as did 38 percent of dentists, 43 percent
of optometrists, and 78 percent of nurse practitioners.
Figure 8: Insurance Acceptance by Provider Type in the NJ 2017 Health Information Technology Survey.
There was heterogeneity among specialties in terms of insurance acceptance. All responding physicians or nurse
practitioners working in Hematology, Hepatology, Nephrology, and Neurosurgery reported accepting
Medicaid/CHIP in their reporting location. More than three quarters of physicians and nurse practitioners in
Anesthesiology did the same (88 percent), as did Oncology (86 percent), Emergency Medicine (82 percent),
Pediatrics (80 percent), Cardiology (79 percent), and Family Medicine (78 percent) reported accepting
Medicaid/CHIP.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
12
Figure 9. Specialists accepting Medicaid/CHIP in the NJ 2017 Health Information Technology Survey.
When thinking of their current patient populations, the median physician estimate was that 20 percent of their
patient or client population was insured by Medicaid (IQR: 30). The median estimate for dentists was 40 percent
(IQR: 50), optometrists was 32.5 percent (IQR: 50), and nurse practitioners was 35 percent (IQR: 50). The
specialties with the highest estimated median percentages of their patient or client population insured by
Medicaid were hepatology (50 percent), psychiatry (29 percent), and pediatrics (26 percent).
Use of Electronic Health Records
A majority of all providers reported using electronic systems for both billing purposes and for maintaining all
health records in their practices. Almost nine in 10 (88 percent) providers currently submit claims electronically,
and the majority of reporting locations across the State of New Jersey (62 percent) use only electronic health
records (EHR) rather than paper ones. Another 22 percent of providers reported that only some of their health
records are electronic, and the rest are on paper. Only 2 percent of providers reported that the reporting
location previously used an EHR but did not currently. Finally, 15 percent reported that the reporting location
had never used an EHR. With the exception of dentists, a majority of physicians (67 percent), optometrists (53
percent), and nurse practitioners (65 percent) reported that all of their health records were electronic. Only 30
percent of dentists reported the same. Thirty one percent of dentists, 25 percent of nurse practitioners, 19
percent of optometrists, and 19 percent of physicians’ reporting locations had some electronic health records
and some on paper. In terms of not using an EHR, 38 percent of dentists, 21 percent of optometrists, 13 percent
of physicians, and 9 percent of nurse practitioners reported that their reporting location had never used an EHR
system. A miniscule proportion of providers reported that their reporting location previously used an EHR but no
longer did: 7 percent of optometrists, and 1 percent each of physicians, dentists, and nurse practitioners.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
13
Electronic
57%
Electronic
and paper
39%
Not used
any EHR
4%
Figure 10. EHR Use by Provider in the NJ 2017 Health Information Technology Survey.
Most providers whose reporting location is a
hospital (either in inpatient or outpatient
settings) used at least some sort of EHR
technology. Fifty-seven percent reported that all
of their health records were electronic; 39
percent reported that the type of health records
are mixed: some electronic, and some on paper.
Finally, four percent of providers in hospitals
declared that their reporting location had never
used an EHR.
Among providers using EHR, most had been
using them for three or more years. Most
providers (78 percent) reported having used any
EHR system for more than three years, while 10
percent said that they have used an EHR for 2-3
years, 7 percent for 1-2 years, and 5 percent for
under one year.
Providers across New Jersey reported currently
using many different EHR systems. The most often used systems were Epic (13 percent) and Cerner (9 percent).
Allscripts, NextGen, and Athenahealth were each reported to be used 5 percent of the time, respectively. Nearly
half of all providers (49 percent) installed their current EHR system in the past five years (since 2012), and an
additional 25 percent had their current EHR system installed in the past ten years. Most providers reported
continuity in their EHR usage over time: over the past ten years, 61 percent of providers reported having used
only one EHR system, 28 percent having used two, and 10 percent having used three to five different systems.
Figure 11. Hospital-based Providers’ EHR Use of Electronic,
Mixed (Electronic and Paper), or None in the NJ 2017 Health
Information Technology Survey.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
14
Very
Satisfied
28%
Somewhat
Satisfied
48%
Somewhat
Dissatisfie
d 15%
Very
Dissatisfie
d 9%
EHR not
Certified
31%
EHR
Certified in
2015
28%
EHR
Certified in
2014/2015
24%
EHR
Certified in
2014
17%
Approximately one third (30 percent) of providers reported that the reporting location had to decide between
buying necessary medical equipment and their EHR system.
Satisfaction with and Capabilities of EHR System
Providers were mostly satisfied with their current EHR system. Twenty-eight percent reported being “very
satisfied” with their EHR, and another 48 percent reported being “somewhat satisfied.” Another 15 percent
reported being “somewhat dissatisfied,” and 9 percent “very dissatisfied.” A majority of those in a solo or group
practice (61 percent) said that they would buy their current EHR again.
Only one quarter of providers (25 percent)
reported that they “strongly agreed” that their
EHR system(s) currently in use at the reporting
location met their clinical needs, while 48 percent
responded “somewhat agree.” Fifteen percent and
11 percent, respectively, said that they “somewhat
disagree” and “somewhat agree” with the
statement.
In terms of EHR capabilities, 45 percent of
providers reported that their EHR had the
capability to electronically send health information
to another provider whose EHR system is not the
same as theirs.
Among all providers, 32 percent reported that
their current EHR was not certified according to
the criteria set forth by the Office of the National
Coordinator for Health Information Technology
(ONC). Another 28 percent reported that their EHR
was certified in the 2015 Edition, 24 percent in the
2014/2015 Edition, and 17 percent in the 2014
Edition.
In terms of future plans with an EHR, only 16
percent of providers conveyed that there were
plans to install a new EHR system in the next 18
months at the reporting location; another 16
percent said that it was a possibility. These future
plans are not dependent on whether the
responding sample of providers have or do not
already have an EHR system.
Figure 12. Provider Satisfaction with their Electronic Health
Record systems in the NJ 2017 Health Information
Technology Survey.
Figure 13. ONC Certification Rates for Providers’ EHRs
according to the NJ 2017 Health Information Technology.
Survey.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
15
Made an
Assessment
79%
Not had an
Assessment
21%
Privacy and Security Risk Assessment
The vast majority of providers (79 percent)
reported that their reporting location had made
an assessment of the risks and vulnerabilities of
their practice’s electronic health information in
the past year, and 21 percent reported they had
not.
Figure 14. Risk Assessments Completion Rate according to
the NJ 2017 Health Information Technology Survey.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
16
Barriers to Using an EHR
Providers reported an array of reasons for not using an EHR. While the majority said that they did not know
precisely why they did not use an EHR, 43 percent said that they did not use one because of the additional costs
necessary to accomplish reporting. Other reasons included the fact that the systems would be too time
consuming for employees (37 percent), the cost of connecting with outside systems (29 percent), technical
difficulties with connecting with outside systems (27 percent), data privacy concerns of the reporting location
(26 percent), EHR vendors not understanding the provider’s needs (25 percent), lack of incentive funding (22
percent), the EHR would be too technical for employees (22 percent), the lack of established national standards
(20 percent), data privacy concerns on the part of the patients (20 percent), inability to train staff (13 percent),
other providers are not using EHRs (11 percent), and a fear of litigation arising from the use of the EHR (9
percent).
Figure 15. Percentages of Barriers Providers Reported For Not Using an EHR in the NJ 2017 Health Information
Technology Survey.
For those that selected more than one reason for not having an EHR, the most often chosen reason (39 percent)
was the cost of the system as the main concern. Another 11 percent said that electronically exchanging health
information is too time consuming for employees, and 10 percent said that EHR vendors do not understand the
clinical needs and workflow of the reporting location.
Prevalence of Other Health Information Technologies
EHR is not the only technology used in providers’ practices: 22 percent reported using medical scribe
technology, and 28 percent reported the use of medical speech recognition technology. Almost all (92 percent)
reported that their reporting location had access to affordable high-speed internet. Other technologies reported
in respondents’ practices included e-prescribing, electronic scheduling, digital imaging, and patient portals,
among other technologies.
Results from this Environmental Scan may support the work that the New Jersey Health Care Quality Institute
(NJHCQI) and The Nicholson Foundation are working on as part of their "Medicaid 2.0: Blueprint for the
Future."
vii
These institutions’ March 2017 release suggests that the "State should foster the expansion of the use
43
37
29
27
26
25
22
22
20
20
13
11
9
0 5 10 15 20 25 30 35 40 45 50
Additional Costs necessary to accomplish reporting
Time consuming
Cost of connecting with outside systems
Technical Difficulties connecting with Outside systems
Data Privacy of reporting location
EHR vendors not understanding the provider's needs
Lack of incentive funding
EHR would be too technical for employees
Lack of established National standard
Data Privacy concerns on the part of the patients
Inability to Train staff
Other providers are not using EHR
Fear of Litigations arising from the use of EHR

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
17
of telehealth and establish demonstration programs in Medicaid to evaluate the use of telehealth to improve
access to specialty care, especially physician to physician eConsults and Project ECHO." One clinician in the
survey responded, "Telehealth is used extensively for everything from genetic testing to pre-op clearance and
home monitoring."
Health Information Exchange
Out of all providers (419 responses), only 18 percent reported participating in a Health Information Exchange
(HIE) platform. This included 21 percent of physicians, 3 percent of dentists, 16 percent of optometrists, and 10
percent of nurse practitioners.
Figure 16. Percentage of HIE Connected Providers among Survey Respondents.
Of those respondents who had an HIE, 16 percent reported that they were “very satisfied” with how it met their
practice’s clinical needs. Another 48 percent were “somewhat satisfied,” 24 percent were “somewhat
dissatisfied,” and 12 percent were “strongly dissatisfied.”
Figure 17. HIE Satisfaction Rates Among Survey Respondents.
0
5
10
15
20
25
30
35
40
45
50
55
Physicians Dentists Optometrists Nurse
Practitioners
Total
Percentage of HIE Connected Providers
Among Survey Respondents

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
18
Forty-eight percent of respondents reported that the HIE’s patient portal was useful in meeting their practice’s
needs; 34 percent and 27 percent said the same regarding hospital integration services and physician integrated
services, respectively. Twenty-four percent found the HIEs’ direct secure messaging tool to be useful. Twenty-
one percent of respondents said that the central repository and portal query/clinical review were useful in
meeting their practice’s clinical needs. Others found that the reporting and statistics (20 percent), security and
compliance (20 percent), virtual practice (10 percent), ADT notifications (8 percent), and master person/patient
index (4 percent) were useful in meeting their practice’s clinical needs. One-fifth of respondents (20 percent)
said that they did not find the HIE services useful.
Providers not sharing patient or client information through HIE had numerous reasons for not participating in an
HIE. Many providers did not have access to an HIE platform (35 percent), did not know how to use an HIE (26
percent), found that the HIE was too technical (22 percent), or that the HIE was too time consuming (22
percent). Providers also cited other providers not using HIEs as their reason for not participating (20 percent),
privacy concerns (19 percent), or that the HIE was not needed (16 percent).
Figure 18. Percentage of Provider Reasons for Not Participating in a Health Information Exchange in the NJ 2017
Health Information Technology Survey.
Medicare/Medicaid Meaningful Use
More than nine in 10 respondents (92 percent) reported that their current EHR system meets Meaningful Use
criteria as defined by the Department of Health and Human Services. Forty-eight percent of providers felt that
financial incentives to advance health information technology were “very important,” and another 34 percent
felt that they were “somewhat important.” Ten percent said that financial incentives to adopt health
information technology were “not very important,” and 8 percent said that they were “not at all important.”
In terms of Meaningful Use incentive payments, 52 percent of respondents reported that their reporting
location had applied for the payments, and an additional 6 percent intended to apply; 3 percent of respondents
were uncertain if they would apply. Another 24 percent of respondents knew of the Meaningful Use incentive
payments but are uncertain of their reporting location’s status with the payments.
35
26
22
22
20
19
16
Did not have access to an HIE platform
Did not know how to use HIE
HIE was too technical
HIE was too time consuming
Other providers not using HIE
Privacy Concerns
HIE was not needed
0 10 20 30 40

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
19
Figure 19. Percentage of Meaningful Use EHR Incentive Participants Among Survey Respondents.
Regarding Stage 3 incentive payments, 40 percent of respondents worked in a location that had applied for
those payments, but another third of respondents (32 percent) did not know what they were. Sixteen percent of
respondents knew what they were but are uncertain of their status. Eleven percent of respondents were
uncertain if they would apply, and 2 percent said that they would not apply.
Figure 20. Percentage of Meaningful Use Stage 3 Incentive Payment Status Among Survey Respondents.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
20
Electronic Health Data Capabilities
The capabilities of the reporting location’s electronic health data capabilities were robust and used routinely.
The majority of respondents reported that their reporting location had computerized capabilities to record a
patient’s medications and allergies, record patient demographics (89 percent), send prescriptions to the
pharmacy (73 percent), and have the ability to provide a patient portal (50 percent); these features were used
routinely.
The capability of identifying educational resources for patients’ conditions (49 percent), reporting clinical quality
measures to federal or state agencies such as CMS or Medicaid (47 percent), the capabilities to do consults
related to diagnosis, testing, or treatment (36 percent), to report to immunization registries (28 percent), and
conducting e-consults for any health-related service, including diagnosis, testing, or treatment of physical or
mental human disease or dysfunction (22 percent), were used routinely.
Figure 21. EHR Capabilities in the NJ 2017 Health Information Technology Survey.
A small percentage of respondents reported that patients seen at their reporting location could engage in many
different activities related to their healthcare in an online setting patients could both request appointments and
enter health information online. Nineteen percent reported that patients could request prescription refills
online, 14 percent had the ability to ask the provider questions online and 11 percent were able to request
referrals. Only 5 percent of respondents reported that patients had the ability to upload data from self-
monitoring devices.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
21
Figure 22. Online Capabilities for Patients in the NJ 2017 Health Information Technology Survey.
Sharing Patient or Client Health Information
Providers reported sharing patient or client health information with other healthcare providers and
organizations: 67 percent reported sharing information with providers in their office or group, 55 percent with
providers outside of their group, 39 percent with hospitals in which the provider is affiliated, 18 percent with a
quality data reporting service, 17 percent with the New Jersey Department of Health, 15 percent with behavioral
health providers, 14 percent with hospitals with which the provider is not affiliated, 12 percent with home
health providers, 8 percent with Health Information Exchanges, and 7 percent with other federal, state, or city
agencies. Only 8 percent of providers reported that they do not share patient or client health information with
other providers.
Providers share health information both electronically and non-electronically with others. Overall, more than a
third of providers sent patient health information to other providers via fax (36 percent) or email (19 percent).
Other providers reported most often sending patient health information to other providers through the other
entity’s EHR (33 percent), and another 26 percent via their own EHR (non-Health Level 7 (HL7) capability).
Nineteen percent reported using direct secure messaging, while 14 percent reported using an HIE portal, and 13
percent reported using postal mail. Eleven percent reported using an interface with the organization other than
an EHR, and 4 percent used a HL7 interface on the EHR.
Electronic Data Sharing
Among providers sharing data electronically, most shared comprehensive patient information. Most shared lab
results (88 percent), imaging reports (84 percent), medication lists (83 percent), patient problem lists (82
percent), and medication allergy lists (77 percent). However, only about a half of providers (51 percent) shared
this type of information using a Summary Care Record, which is an electronic file with these data in electronic
format.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
22
Figure 23. Types of Information and Data Sharing Rates among Providers who Share Electronic Information in
the NJ 2017 Health Information Technology Survey.
For providers sharing patient health information with affiliated hospitals or unaffiliated hospitals, 41 percent
reported that they were always electronically sent directly from their EHR to hospital’s EHR system; another 19
percent said that patient information was “often” sent, 19 percent said that patient information was
“sometimes” sent, 6 percent said that patient information was “rarely” sent, and 16 percent reported that it was
“never” sent.
Discharge Summaries
Among the providers who reported electronically sharing patient information with affiliated or unaffiliated
hospitals, 78 percent took care of patients after they were discharged from an inpatient setting. Of these
providers, 32 percent reported “always” receiving a discharge summary from the hospital with clinical
information; another 32 percent and 23 percent reported that they “often” or “sometimes” received this
information, respectively. Five (5) percent reported that they “rarely” received a discharge summary with clinical
information, and 9 percent reported that they “never” received this information. Of those receiving a discharge
summary, most received the summary electronically at least some of the time (26 percent “always,” 36 percent
“often,” 13 percent “sometimes,” and 8 percent “rarely”). The remaining 18 percent reported that they rarely
received discharge summaries electronically.
Electronic discharge records were largely distributed via the hospital’s EHR system (47 percent), with another 34
percent via the provider’s EHR, 16 percent with an interface other than the hospital’s EHR (16 percent), and 13
percent through an HIE portal. When receiving these discharge summaries from affiliated or unaffiliated
hospitals, 41 percent of respondents reported being able to automatically incorporate the information into their
EHR.
88
84
83
82
77
51
Most Shared Lab results
Imaging Report
Medication Lists
Patient Problem Lists
Medication Allergy Lists
Providers Shared information
using Summary Care Record
0 20 40 60 80 100

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
23
Preferences for Future Electronic Data Sharing
When considering the type(s) of patient or client data that their reporting location currently received,
respondents suggested various types of additional patient or client data that they would like to receive
electronically but currently do not. Many providers expressed a desire to receive imaging, lab results, and other
test results; most did not know why their reporting location was not able to receive the electronic healthcare
data they desired at this time.
Among all respondents, 59 percent reported wanting to participate in statewide data sharing, and 72 percent of
respondents reported wanting to electronically share data with out-of-state providers. In terms of facilitating
that data sharing with healthcare stakeholders such as providers, hospitals, HIEs, payers, and the New Jersey
Department of Health, many respondents suggested a standardized interface with access to others providers’
EHRs.
Though 8 percent of respondents reported already receiving electronic Admission, Discharge, or Transfer (ADT)
notifications, 51 percent expressed a desire to receive them; another 17 percent said they would not like to
receive them. Less than 10 percent of respondents reported already electronically querying the New Jersey
Immunization registry, and more than half of respondents (52 percent) would like to be able to query the
registry. Of the 262 physicians answering, 50% reported wanting to query the NJ Immunization Registry, as did
23% (N=39) of dentists, 22% (N=32) of optometrists, and 55% (N=139) of NPs. Thirty-nine percent of
respondents did not wish to have the ability to electronically query the immunization registry. Finally, 12
percent of respondents reported that they already submitted their patients’ immunization records electronically
to the immunization registry. Respondents were split between submitting (44 percent) and not submitting (44
percent) to the registry.
Medical Home Model and Alternative Payment Model
With regards to the Agency for Healthcare Research and Quality (AHRQ)’s Medical Home model, only 14 percent
of respondents reported that their reporting location receives additional compensation beyond routine visit fees
for providing Patient Centered Medical Home (PCMH) type services, or for participating in a certified PCMH
arrangement. One quarter (25 percent) of respondents’ reporting locations reported participating in a Pay-for-
Performance arrangement, where it can receive financial bonuses based on performance. Reporting locations
submitted their Quality Measures Performance data to Medicare,
Medicaid, and/or other plans at various intervals.
Twenty-five percent reported submitting the data once a year, 7 percent two times a year, 16 percent more
than two times a year, and 30 percent did not submit quality measures to Medicare/Medicaid. Reporting
locations typically submitted a median of five Quality Measures (IQR: 8) to Medicare, Medicaid, and/or other
plans. In terms of the reporting location’s EHR capabilities, 42 percent of respondents said that their EHR was
able to produce reports and performance data on the Quality Measures desired by the provider; 21 percent said
their EHR did not accomplish this. A plurality of respondents (37 percent) reported not knowing what reports
and performance data they would like. Finally, 30 percent of respondents reported that their reporting location
participated in an Accountable Care Organization (ACO) or similar APM arrangement.
Demographics
Seventy (70) percent of survey respondents were aged 50 or older, and exactly half were female.
Nearly all respondents were providers themselves (93 percent); only 7 percent of respondents were the office
manager or practice staff member. All New Jersey counties were represented in the survey.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
24
Providers affiliated with Community Health Centers (Federally Qualified Health Centers (FQHC))
The vast majority of respondents (77 percent) whose reporting locations were Community Health Centers
(including FQHCs, federally-funded clinics, or “look-alike” clinics) reported using entirely electronic health
records, and an additional 15 percent reported that some of their reporting location’s health records were
electronic. Three percent of respondents reported that their reporting location used to have an EHR but do not
any longer, and the remaining 5 percent of respondents reported that their reporting location has never used an
EHR.
Ninety-four percent of respondents reported working in reporting locations that meet Meaningful Use criteria as
defined by the Department of Health and Human Services, to the best of the respondent’s knowledge. Thirteen
percent of Community Health Centers participate in an HIE.
Broadband Internet Access
Quick Statistics
o In total there are 94 broadband providers in New Jersey.
o Everyone in New Jersey has access to some form of broadband.
o There are 130,000 people in New Jersey that have access to only one wired provider, leaving them
no options to switch.
o Another 35,000 people in New Jersey do not have any wired internet providers available where they
live.
o 2 percent are underserved (less than 2 wired providers).
o 41.3 Megabits per second (MBPS) Average Download Speed (7/28/2015).
o 3rd most connected state based on percentage of population with broadband access.
Broadband Access
Figure 24. Access to Broadband Internet in NJ. Figure 25. Broadband Speed Availability.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
25
Federally Qualified Health Centers (FQHCs)
All of the 23 Federally Qualified Health Centers (FQHCs) that NJII is working with in state of NJ are on Modified
Meaningful Use (MU) Stage 2 for EHR. All FQHCs in New Jersey must be on Modified MU Stage 2 per regulations.
These FQHCs have a number of satellite offices throughout New Jersey.
Figure 26. Number of Community Health Center such as Federally Qualified Health Center (FQHC), federally-
funded clinics, “look-alike” clinics, or satellite locations distributed by County in NJ.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
26
Health Information Exchange Presence in New Jersey
The New Jersey Health Information Network (NJHIN) is owned and funded by New Jersey Department of Health
(NJDOH) and managed by the New Jersey Innovation Institute. NJHIN provides the infrastructure for electronic
exchange of patient health information among Health Information Exchange Organizations and State health data
sources. It also is the primary vehicle for New Jersey to eventually exchange health information nationally.
New Jersey has numerous regional Health Information Exchange Organizations (HIEs/HIOs) and integrated
delivery networks (IDNs) that are all operating to support health information exchange in the state. There are
also six Designated Health Information Organizations throughout New Jersey. While there are numerous options
for organizations to participate, there is still approximately 30 Hospitals that do not participate in any HIOs.
17
3
32
3
4 4
0
5
10
15
20
25
30
35
Camden
Coalition of
Healthcare
Providers
Highlander
Health Data
Network
Jersey Health
Connect
NJSHINE Trenton
Health Team
Virtua Health
Hospitals connected to the HIE
785
1,200
6,000
900
650
500
0
1000
2000
3000
4000
5000
6000
7000
Camden
Coalition of
Healthcare
Providers
Highlander
Health Data
Network
Jersey Health
Connect
NJSHINE Trenton
Health Team
Virtua Health
Users connected and using HIE Services

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
27
Figures 27a-d. Hospitals Connected to the HIE; Users connected and using HIE Services; Unique patients
contained in system; Patient portal users.
800,000
500,000
6,500,000
800,000
300,000
1,421,390
-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
Camden
Coalition of
Healthcare
Providers
Highlander
Health Data
Network
Jersey
Health
Connect
NJSHINE Trenton
Health Team
Virtua
Health
Unique patients contained in system
0 0
250,000
275,000
0
24205
0
50000
100000
150000
200000
250000
300000
Camden
Coalition of
Healthcare
Providers
Highlander
Health Data
Network
Jersey Health
Connect
NJSHINE Trenton
Health Team
Virtua Health
Patient HIE portal users

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
28
NJ HIE Core Services
*In this table and the following tables, “Adoption” meaning member participation in the service is measured
“High” by meeting a 65% or above threshold, while “Low” meets 64% or below threshold. ‡Roadmap items
mean that this service is on the HIO’s high level timeline of the organization's goals and deliverables. †Pilot
means that this service is in a testing phase. “NA” means not applicable.
NJ HIE Advanced Services
Advanced Services
NJSHINE
Trenton
JHC
Highlander
Camden
Virtua
CONNECT & NwHIN
Protocols - XCA, etc.
Low
Adoption
NA
Roadmap
NA
Low
Adoption
Pilot
Direct Messaging
Low
Adoption
Low
Adoption
Low
Adoption
Low
Adoption
Low
Adoption
Low
Adoption
Encounter
Notification
Pilot
High
Adoption
High
Adoption
Roadmap
High
Adoption
NA
Patient Portal
High
Adoption
Low
Adoption
High
Adoption
Low
Adoption
NA
Low
Adoption
Virtual Practice
Low
Adoption
NA
High
Adoption
NA
NA
NA
Core Services
NJSHINE
Trenton
JHC
Highlander
Camden
Virtua
HIE
Infrastructure and
Central Repository
High
Adoption*
High
Adoption
High
Adoption
Roadmap ‡
High
Adoption
High
Adoption
Hospital Integration
Services
High
Adoption
High
Adoption
High
Adoption
High
Adoption
High
Adoption
High
Adoption
MPI (Regional)
Pilot †
High
Adoption
NA
NA
High
Adoption
High
Adoption
MPI (Statewide)
NA
High
Adoption
NA
NA
Roadmap
Roadmap
Physician Integration
Services
High
Adoption
Low
Adoption
High
Adoption
Roadmap
Roadmap
Low
Adoption
Portal Query and
Clinical Review
High
Adoption
High
Adoption
High
Adoption
Low
Adoption
High
Adoption
Roadmap
Reporting and
Statistics
High
Adoption
High
Adoption
Low
Adoption
Roadmap
Low
Adoption
Low
Adoption
Security and
Compliance Program
High
Adoption
High
Adoption
High
Adoption
High
Adoption
High
Adoption
High
Adoption

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
29
NJ HIE Value Services
Value Services
NJSHINE
Trenton
JHC
Highlander
Camden
Virtua
Active Care
Relationships
Database
Low
Adoption
Low
Adoption
NA
NA
Roadmap
NA
ADT Notification
(Regional)
High
Adoption
High
Adoption
High
Adoption
Roadmap
High
Adoption
NA
ADT Notification
(Statewide)
NA
High
Adoption
Roadmap
Roadmap
Low
Adoption
NA
Alerting (based on
rules)
Low
Adoption
High
Adoption
Roadmap
Roadmap
High
Adoption
NA
Clinical Data
Integration Services
High
Adoption
High
Adoption
High
Adoption
Roadmap
High
Adoption
NA
Core Consulting for
Value based Programs
Low
Adoption
Low
Adoption
NA
NA
Roadmap
NA
Educational Services
Roadmap
High
Adoption
Low
Adoption
Roadmap
NA
NA
Immunization Registry
Query by Parameter
(QBP)
Roadmap
NA
Roadmap
Roadmap
Roadmap
NA
Immunization Registry
Summit
Roadmap
NA
NA
NA
Roadmap
NA
Medicaid Provider
Program
NA
Roadmap
NA
NA
Roadmap
NA
Participation in
National HIE
Collaborative (SHIEC)
Roadmap
NA
High
Adoption
NA
Roadmap
NA
Practice
Transformation
Services (CMS PTN)
Low
Adoption
NA
NA
NA
NA
NA
Public Health
Reporting for MIPS
Pilot
NA
NA
NA
Roadmap
NA

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
30
New Jersey Health Information Exchange Organizations
Camden HIE
The Camden Health Information Exchange (HIE) was launched in 2010 by the Camden Coalition of Healthcare
Providers and is the result of a collaborative data sharing effort to improve care delivery in Camden. The original
founders of the HIE are Cooper Health System, Virtua, and Our Lady of Lourdes Health System. The HIE is
currently used by over 100 healthcare providers in Camden. Camden HIE is also a Medicaid ACO.
Greater Healthy Newark (Highlander Health Data Network)
The Greater Healthy Newark Team is a community health improvement collaborative serving Newark, NJ. The
collaborative is an innovative partnership among University Hospital, Newark Beth Israel, St. Michaels and East
Orange Medical Centers. The HIE is also a Medicaid ACO and supports beneficiaries from several zip codes in
Newark, NJ.
Jersey Health Connect
Jersey Health Connect is New Jersey's largest HIO and has approximately half of the health systems and
hospitals of New Jersey connected to their HIE platform. In addition, several long term and post-acute care
(LTPAC) facilities and provider practices are directly connected to JHC and participating in data exchange.
NJSHINE
NJSHINE facilitates health information exchange for the diverse populations of a seven-county region in South
Jersey to improve the quality of care, support patient safety, facilitate care coordination across the continuum of
care, reduce cost, and improve patient outcomes. Hospitals connected through NJSHINE include Shore Medical
Center, Underwood Memorial Hospital, Cape Regional Medical Center, and Inspira Medical and Health Centers.
NJSHINE also connects other area health providers like long-term care facilities and rehabilitation centers.
Trenton HIE
The Trenton Health Team is a community health improvement collaborative serving Trenton, NJ. The
collaborative is an innovative partnership among St. Francis Medical Center, Capital Health, Henry J. Austin
Federally Qualified Health Center and the Department of Health and Human Services of the City of Trenton. The
vision of the Trenton Health Team is to make Trenton the healthiest city in the state, with a mission to transform
healthcare for the city by forming a committed partnership with the community to expand access to high
quality, coordinated healthcare, while being ever mindful of the necessity of containing and saving costs.
Virtua HIE
The Virtua HIE is operated by Virtua Health, Inc. and serves Burlington, Camden, and Gloucester counties, with
free membership to any healthcare organizations therein, thereby making it a community service activity. The
Virtua HIE strives to offer a comprehensive set of health records, presented in a longitudinal, patient-centric
manner. Such records may be viewed via a web-based portal, or members may elect to have the records
interfaced directly into their electronic health records. The Virtua HIE’s strategy includes close adherence to
national interoperability standards (as published periodically by ONC and the non-profit standards organization
called Integrating the Healthcare Enterprise), and it has sophisticated mechanisms to meet Federal and State
regulations on the release of “sensitive” data.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
31
State Activities to Facilitate HIE and EHR Adoption
The New Jersey Health Information Network
The NJHIN as stated previously provides the infrastructure for electronic exchange of patient health information
among Health Information Exchange Organizations and State health data sources. The New Jersey Department
of Health (NJDOH) partnered with the New Jersey Innovation Institute (NJII) as the State Designated Entity on an
ONC grant to “Advance Interoperable Health Information Technology Services to Support Health Information
Exchange” that was awarded in July 2015 and will run through July 2017.
Beginning with a pilot initiative that includes the Highlander HDN and its participating organizations in the
Newark metropolitan area, NJDOH and NJII have established an NJHIN Shared Services Platform that includes
the following services:
• A statewide Master Person Index (MPI), allowing NJ Residents to be uniquely identified across the
healthcare continuum. Open APIs allow for real-time integration into across systems and
organizations.
• A statewide Admission, Discharge, and Transfer (ADT) Notification Service that sends alerts to
providers and care management teams on a patient’s status, improving post-discharge outcomes,
prompting follow up care, and improving communication among providers.
• A Common Key Service (CKS) that provides a consistent and reliable way to uniquely identify and
match patients across multiple organizations, applications, and services, thereby improving patient
safety and data integrity
• A Health Directory Service that manages information on organizations and their associated
healthcare professionals, including provider preferences for receiving healthcare information.
• A State Health Data Hub that allows providers of participating HIOs to query health information
from, and, in some cases, submit health information to, state health systems such as the New Jersey
Immunization Information Systems (NJIIS), the state’s immunization registry.
The NJHIN core goals are achievable by:
• Uniquely identifying individuals across the state, which ensures accurate and relevant health
information is identified.
• Enabling the exchange and sharing of data across the healthcare continuum, to enable improved
care coordination.
• Simplifying and expanding access to NJ public health registries through a normalized and repeatable
process.
• Educating and outreach to at-risk populations across the state proactively.
• Ensure quality data is shared, the purpose of data exchange hinges on quality not quantity.
As an example, the NJHIN shares some commonalities with a Health Information Exchange Organization but
there are also differences between what a Health Information Network is intended to provide in New Jersey
compared to what an HIO (Jersey Health Connect (JHC)) may provide in New Jersey.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
32
Figure 28. Jersey Health Connect Service Catalog and NJHIN Comparison.
HIO/HIE Activities across State Borders
The New Jersey Health Information Network is currently working with the Delaware Health Information Network
(DHIN) on connecting the two regional Health Information Networks. This connection is initially intended to
support the NJHIN ADT Notification Use Case. The NJHIN and New Jersey Department of Health (NJDOH) are
currently in conversation on connectivity to nearby states Pennsylvania, New York, and Maryland. The HIO,
NJSHINE, has established a connection to DHIN to allow for the notification of NJSHINE participants that seek
care in Delaware.
HIO/HIE Interoperability
The current HIO environment in the state does not support state wide data sharing or collaborations between
entities. With the successful launch of the NJHIN the infrastructure and legal framework is now in place to allow
the collaboration and data sharing state wide across all HIOs. By implementing specific Use Cases NJHIN will
enable purpose driven use cases to move forward data sharing to improve patient outcomes and allow
interoperability between the disparate systems.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
33
Conclusion: Key Findings
The New Jersey Innovation Institute identified key findings that should be further researched and specifically
targeted in the State Medicaid Health Information Technology Plan (SMHP).
EHR Adoption
Although up to 86% of physicians are using some form of EHR based on full or partial adoption, the fact that
potentially up to 33% of physicians are still using paper charts would indicate room for improvement with regard
to increasing the full adoption of electronic health record systems in practices. There is a lower adoption of EHRs
and HIT by specialists, especially dentists (total of 61% full or partial EHR adoption) and optometrists (total of
72% full or partial EHR adoption), which could be a target for improvement. Optometrists had the higher than
normal abandon rate of EHRs (7%) than the other provider types (physicians, nurse practitioners, and dentists
were at 1%), so education and training may help to improve adoption rates. At 90% of full or partial EHR
adoption, nurse practitioners excelled in terms of adopting EHR systems. Overall, 83% of total providers
surveyed have either fully or partially adopted an EHR system.
Although the vast majority of providers (79%) had performed risk assessments of the potential risks and
vulnerabilities of their practice’s electronic health information in the past year, the fact that 21 percent reported
not having done so poses a significant HIPAA compliance issue. Moreover, among those who did not use EHRs,
up to 43% said are not using one because of the perceived additional costs necessary to accomplish reporting (of
measures to payers). In general, providers found costs to be the main barrier to the adoption and use of EHR
and/or HIT.
Health Information Exchange
There are low level of health information exchange activities occurring throughout the state of NJ. The NJHIN
should be leveraged to promote open connectivity and appropriate sharing of health Information. Providers may
not be aware or may be confused about the ability to join and access HIE services. The results surrounding the
sharing of patient or client health information seem to be lower than one might expect. Only two-thirds (67%) of
providers are sharing information with providers in their office or group while a little more than half of providers
share data with providers outside of their group, and two-fifths (39%) share data with hospitals in which the
provider is affiliated. There are State requirements for submission of certain data to the New Jersey Department
of Health, but less than a fifth of respondents seem to submit data to the NJDOH. As not every practice is
integrated with an HIE, it is understandable that only 8% of practices are exchanging data with an HIE. Among 70
respondents, 41% said they always send information directly from their EHR to another EHR, and only 19% are
often or sometimes sending this information. Respondents positively suggested that having standardized
interfaces with access to others providers’ EHRs would be helpful.
However, one might have expected for more practices to be recipients of data exchanged electronically
(excluding fax) and not necessarily have the technologies abilities to send data out if interfaces are not set up
with external entities. Nonetheless, more education about interoperability (“ability of different information
technology systems and software applications to communicate, exchange data, and use the information that has
been exchanged”)
viii
and how patient data is being shared is needed to encourage increased adoption and use of
HIE technologies within providers’ daily clinical workflows. The NJHIN and HIEs are collaborating on better and
consistent patient identification solutions across disparate systems to uniquely identify patients and reduce
redundant and inappropriate services that may be rendered in healthcare settings. The ongoing effort to
connect disparate organizations must include an emphasis on data quality to ensure that the right information is
delivered at the right time and to the right persons who are best positioned to coordinate care for patients. The
NJHIN Use Case framework allows for normalized and validated data from trusted sharing organizations to be

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
34
more timely and easier to access for providers. Stakeholders may also employ predictive analytics to derive
meaningful conclusions from data to inform better clinical decisions.
Health Information Technology
There are low levels of adoption of health information technologies as indicated by the low rate (below 30% in
general) of the use of scribe, medical speech recognition, and telehealth-related technologies. Responses among
those using HIT indicated openness to using varying types of technologies to accomplish different clinical
functions, especially where clinical operations are integrated with communication, prescribing, dispensing,
monitoring, laboratory, and imaging devices and technologies. The potential to achieve greater efficiencies and
outcomes in the delivery of care to patients is a strong reason why healthcare organizations are actively
promoting telehealth and other existing HIT capabilities.
Broadband Coverage
New Jersey has significant broadband coverage, and this strong network of coverage could be leveraged in
conjunction with NJHIN Use Cases to increase mobility and accessibility for healthcare stakeholders to
participate in exchanging health information.
Education
Based on the overall survey findings, there is a strong need for better education for all provider types. Special
focus should especially be on areas of security and HIPAA compliance, data quality, interoperability as far as
electronically sharing data outside of one’s office, and general HIT and electronic health record education.
Although 78% out of 58 respondents conducted post-discharge follow-up care for patients, one might expect
that more of the providers in this survey would be conducting post-discharge follow-up care. Placing educational
emphasis on the importance of Transitional Care Management could potentially improve this figure.
NJ’s HIT Landscape to Continue to Evolve by Leveraging HIT Capabilities
The need to leverage existing HIT capabilities is paramount. There has been tremendous state and federal
investments in EHRs, HIEs, NJHIN infrastructure and other HIT technologies in New Jersey. There should be a
focus on using the existing capabilities and infrastructure to further increase HIT adoption, interoperability, and
the appropriate sharing of health information.

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
35
Appendix A: List of Abbreviations
ACRS – Active Care Relationship Service
ADT – Admit, Discharge, Transfer
BAA – Business Associate Agreement
BCBSNJ – Blue Cross Blue Shield of New Jersey
BOD – Board of Directors
CCD – Continuity of Care Document
CDC – Centers for Disease Control and Prevention
CMR – Computerized Medical Record
CMS – Center for Medicare and Medicaid Services
CDURSA – Consumer Qualified Organization Data Sharing Agreement
CTDSO – Consumer Qualified Organization / NJHIN Consumer Qualified Data Sharing Organization
DHS – Department of Human Services
DOD – Department of Defense
DOH – Department of Health
DQ – Document Query / Document Query Message
DR – Document Retrieve / Document Retrieve Message
DURSA – Data Use and Reciprocal Support Agreement
DUA – Data Use Agreement
EHR – Electronic Health Record
EMR – Electronic Medical Record
eSMD – Electronic Submission of Medical Documentation System
EULA – End-User License Agreement
HIE – Health Information Exchange (as a verb or noun)
HIO – Health Information Exchange Organization (noun)
HIPAA – Health Insurance Portability and Accountability Act
HISP - Health Information Systems Program
HIT – Health Information Technology
HL7 – Health Level 7
Https – Post-to-URL Transport connectivity (Hypertext Transfer Protocol Secure)
IDN – Integrated Delivery Network (such as a health system)
IHE - Integrating the Healthcare Enterprise® (integrated health information profiles)
LLP – Lower Layer Protocol (HL7)
JHC – Jersey Health Connect
NJHIN – New Jersey Health Information Network
NJHIN BOD – New Jersey Health Information Network Board of Directors
NJHINSS – New Jersey Health Information Network Shared Services
NJDOH – New Jersey Department of Health
NJDHS – New Jersey Department of Human Services
NJOAC – NJHIN Operations Advisory Committee
MPI – Master Person Index
MTM – Medication Therapy Management
MU – Meaningful Use
NwHIN – Nationwide Health Information Network
NwHIN SOAP – Nationwide Health Information Network Simple Object Access Protocol
OID – HL7 Organization ID / Unique ID of the Organization
ONC – Office of the National Coordinator
PD – Patient Discovery / Patient Discovery Message

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
36
PHI – Protected Health Information / HIPAA-Protected Health Information
PMP – NJ Prescription Monitoring Program
QA – Quality Assurance
QA Testing – Quality Assurance Testing
TDSO – Trusted Data Sharing Organization / Qualified Organization / NJHIN Qualified Data Sharing Organization
SOAP – Simple Object Access Protocol
SONJ – State of New Jersey
SSA – U.S. Social Security Administration
SSO – Sponsored Sharing Organization
TBD – To Be Determined
URL – Uniform Resource Locator (Internet web site address)
VA – Veterans Administration / U.S. Department of Veterans Affairs
VPN – Virtual Private Network
XAML – Extensible Application Markup Language
XCA – Cross-Community Access
XCPD – Cross-Community Patient Discovery

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
37
Appendix B: HIT Coverage on Geographic Maps of New Jersey
1. New Jersey County Boundaries
ix

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
38
2. New Jersey Hospitals 3. New Jersey FQHCs
New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
39
4. Broadband Coverage by Town
x
Cities
Broadband
Coverage
Cities
Broadband
Coverage
Absecon
95.20%
Long Branch
97.60%
Asbury Park
100.00%
Manchester Township
98.30%
Atlantic City
98.20%
Marlton
99.60%
Bayonne
100.00%
Matawan
100.00%
Belleville
99.50%
Millville
97.60%
Blackwood
98.50%
Monroe Township
99.30%
Bloomfield
99.50%
Montclair
99.50%
Brick
98.30%
Morristown
100.00%
Bridgeton
99.70%
Mount Laurel
96.10%
Bridgewater
99.30%
Neptune
99.50%
Burlington
93.90%
New Brunswick
100.00%
Camden
98.70%
Newark
100.00%
Cherry Hill
97.50%
North Bergen
99.80%
Clementon
99.60%
North Brunswick
99.30%
Clifton
100.00%
Old Bridge
100.00%
East Brunswick
99.30%
Passaic
100.00%
East Orange
99.20%
Paterson
100.00%
Edison
99.30%
Perth Amboy
99.80%
Egg Harbor Township
95.10%
Piscataway
99.30%
Elizabeth
100.00%
Plainfield
99.90%
Englishtown
100.00%
Princeton
100.00%
Fair Lawn
100.00%
Sewell
97.70%
Flemington
98.30%
Sicklerville
97.50%
Fort Lee
100.00%
Somerset
99.40%
Freehold
100.00%
Teaneck
99.90%
Garfield
100.00%
Toms River
99.40%
Hackensack
100.00%
Trenton
99.90%
Hillsborough
99.30%
Union
99.70%
Hoboken
100.00%
Union City
100.00%
Howell
99.50%
Vineland
95.50%
Irvington
99.50%
Wayne
100.00%
Jackson
98.30%
West Deptford
97.70%
Jersey City
99.60%
West New York
100.00%
Kearny
98.60%
West Orange
99.50%
Lakewood
100.00%
Westfield
99.90%
Lawrence Township
98.50%
Williamstown
97.00%
Linden
99.80%
Willingboro
96.10%

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
40
Appendix C: Population Data of New Jersey
Currently, New Jersey has a population of 8,944,469 across 21 Counties as of most recently available figures in
2016.
xi
County
Population
Bergen
939,151
Middlesex
837,073
Essex
796,914
Hudson
677,983
Monmouth
625,846
Ocean
592,497
Union
555,630
Camden
510,150
Passaic
507,945
Morris
498,423
Burlington
449,284
Mercer
371,023
Somerset
333,751
Gloucester
292,330
Atlantic
270,991
Cumberland
153,797
Sussex
142,522
Hunterdon
124,676
Warren
106,617
Cape May
94,430
Salem
63,436

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
41
The Population of New Jersey as of 2016.
New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
42
A Profile of New Jersey’s Physicians
The Meaningful Use EHR Incentive Program for New Jersey
xii
from January 2011 through June 2017 includes:
Unique Count of Eligible Professionals (EPs) 3,193 Medicaid and 9,702 Medicare.
Unique Count of 2 Medicaid Hospitals, 4 Medicare Hospitals, both Medicare and Medicaid 64 Hospitals.
According to the American Medical Association Physician Masterfile of 2014
xiii
, there were the following
amounts of active physicians:
Total Active Physicians:
25,930
Primary Care Physicians:
8,569
Total Residents:
2,875
Total Female Physicians:
9,045
Total Medical or Osteopathic Students:
2,177
By April 2017, the amount of total active physicians in New Jersey increased to 27,923, with primary care
physicians amounting to 13,699 and there were 14,224 specialists according to the Kaiser Family Foundation.
xiv

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
43
Revision History
Version
Date
Comments
1.0
9/18/2017
Final

New Jersey Health Information Technology Environmental Scan
NEW JERSEY INNOVATION INSTITUTE, HEALTHCARE DELIVERY SYSTEMS ILAB
44
References
i
Adoption of Electronic Health Record Systems among U.S. Non-Federal Acute Care Hospitals: 2008-2015
(https://dashboard.healthit.gov/evaluations/data-briefs/non-federal-acute-care-hospital-ehr-adoption-2008-
2015.php)
ii
Hospitals Participating in the Centers for Medicare & Medicaid Services (CMS) EHR Incentive Programs by 2015
(https://dashboard.healthit.gov/datadashboard/documentation/cms-ehr-incentive-program-measures-
documentation.php)
iii
Health IT Data Summaries: New Jersey in 2015 (https://dashboard.healthit.gov/apps/health-information-
technology-data-summaries.php?state=New+Jersey&cat9=all+data)
iv
Health IT Data Summaries: New Jersey in 2015 (https://dashboard.healthit.gov/apps/health-information-
technology-data-summaries.php?state=New+Jersey&cat9=all+data)
v
Cho, Young Ik, Timothy P. Johnson, and Jonathan B. VanGeest. "Enhancing surveys of health care professionals:
a meta‐analysis of techniques to improve response." Evaluation & the health professions 36.3 (2013): 382‐407.
vi
Bethlehem, Jelke. "Selection bias in web surveys." International Statistical Review 78.2 (2010): 161‐188.
vii
NJHCQI and The Nicholson Foundation, “Medicaid 2.0: Blueprint for the Future,” March 2017
(https://thenicholsonfoundation.org/sites/default/files/Medicaid_Blueprint_for_the_Future.pdf)
viii
HIMSS “Interoperability” Definition (http://www.himss.org/library/interoperability-standards/what-is-
interoperability)
ix
NJ County Map and Boundaries (http://geology.com/county-map/new-jersey-county-map.gif)
x
Broadband Statistics in NJ (http://broadbandnow.com/New-Jersey)
xi
NJ State Population: “State Population Totals Tables: 2010-2016”
(https://www.census.gov/data/tables/2016/demo/popest/state-total.html)
xii
Centers for Medicare and Medicaid Services, “Unique Count of Providers By State For Eligible Providers and
Hospitals Paid by The EHR Incentive Program” (https://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/Downloads/June2017_UniqueCountofProvidersbyState.pdf)
xiii
A Profile of New Jersey’s Physicians based on the American Medical Association Physician Masterfile of 2014
and American Association of Medical Colleges 2015 State Physician Workforce Data Book
(https://www.aamc.org/download/447206/data/newjerseyprofile.pdf)
xiv
NJ Active Providers: Kaiser Family Foundation: Total Professionally Active Physicians April 2017
(http://www.kff.org/other/state-indicator/total-active-
physicians/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D)
