
`
Technical Evaluation, Testing, and Validation of the
Usability of Electronic Health Records:
Empirically Based Use Cases for Validating Safety-
Enhanced Usability and Guidelines for Standardization
Svetlana Z. Lowry
Mala Ramaiah
Sheryl Taylor
Emily S. Patterson
Sandra Spickard Prettyman
Debora Simmons
David Brick
Paul Latkany
Michael C. Gibbons
This publication is available free of charge from:
http://dx.doi.org/10.6028/NIST.IR.7804-1
NISTIR 7804-1

Technical Evaluation, Testing, and Validation of the Usability
of Electronic Health Records:
Empirically Based Use Cases for Validating Safety-Enhanced
Usability and Guidelines for Standardization
Svetlana Z. Lowry
Mala Ramaiah
Information Access Division
Information Technology Laboratory
S
heryl Taylor
Software and Systems Division
Information Technology Laboratory
E
mily S. Patterson
The Ohio State University
Columbus, OH
S
andra Spickard Prettyman
Akron University
Akron, OH
D
ebora Simmons
St. Luke’s Health System
Houston, TX
D
avid Brick
NYU Langone Medical Center
New York, NY
P
aul Latkany
New York Eye and Ear Infirmary
New York, NY
M
ichael C. Gibbons
The Johns Hopkins University
Baltimore, MD
This publication is available free of charge from:
http://dx.doi.org/10.6028/NIST.IR.7804-1
U.S. Department of Commerce
Penny Pritzker, Secretary
National Institute of Standards and Technology
Willie May, Acting Under Secretary of Commerce for Standards and Technology and Acting Director
NISTIR 7804-1
October 07, 2015

ii
Acknowledgments
The authors gratefully acknowledge the intellectual contributions from the following:
• Mary Theofanos, M.S., Human Factors Scientist, National Institute of Standards and
Technology
• Brian Stanton, M.S., Cognitive Scientist, National Institute of Standards and Technology
• Kristen Greene, Ph.D., Cognitive Scientist, National Institute of Standards and Technology
• David R. Hunt, M.D., Medical Director, Patient Safety & Health IT Adoption at Office of the
National Coordinator, Office of the Chief Medical Officer
• Teresa Zayas-Caban, Ph.D., Special Assistant to the Deputy National Coordinator , Office of
the National Coordinator
• Ellen V Makar, M.S.N., R.N.-B.C., C.C.M., C.P.H.I.M.S., C.E.N.P., US Dept. of Health and
Human Services, Agency for Healthcare Research and Quality, Center for Evidence and
Practice Improvement
• Michael L. Hodgkins, M.D., M.P.H., Chief Medical Information Officer, American Medical
Association
• Tejal Gandhi, M.D., M.P.H., CPPS, President, National Patient Safety Foundation
• Limor Hochberg, M.S., Human Factors Specialist, Life & Health, UL LLC, Wiklund R&D
• Kelly Cochran, M.S., R.N., Policy Advisor, Health Information Technology, Department of
Health Policy, American Nurses Association
• Mary D. Patterson, M.D., M.Ed., Associate Vice Chair, Medical Education Research in
Simulation, Director of Children's Academy of Pediatric Educators, Children's National
Medical Center
• Janey Barnes, Ph.D., Human Factors Specialist, User-View, Inc.
• Susan Harkness Regli, Ph.D., Human Factors Scientist, University of Pennsylvania Health
System
• Ross Teague, Ph.D., Senior Manager of User Experience, Allscripts Healthcare Solutions,
Inc.
• Hardeep Singh, M.D., MPH, Chief, Health Policy, Quality and Informatics Program,
Houston Veterans Affairs Health Services Research Center for Innovations
• John Ritter, HL7 EHR Work Group co-chair; PHR Work Group co-facilitator; EHR System
Usability Work Group co-facilitator HL7 International Mentoring Committee co-chair ISO
TC/215 U.S. Technical Advisory Group member Western Pennsylvania HIMSS Board of
Director member
• Thomas Elmquist, M.D., Cardiologist, New York Cardiovascular Associates
• Todd C. Hughes, Ph.D., Chief Technology Officer, Next Century Corporation
• Theresa Cullen, M.D., Chief Medical Information Officer, Veterans Health Administration
(VHA)
• Jorge A. Ferrer M.D., M.B.A., Biomedical Informatician, VHA OIA Health Informatics,
Adjunct Assistant Professor, UTHealth School of Biomedical Informatics
• Jan Horsky, Ph.D., Senior Research Scientist, Brigham and Women’s Hospital, Division of
General Internal Medicine and Primary care; Harvard Medical School

iii
In addition, the authors appreciate the access to the data collected under NIST contract number
SB134110CN0107 (UL-Wiklund) and the many instructive contributions from a broad spectrum of
stakeholders on the draft document during an invited stakeholder meeting held at the National
Institute of Standards and Technology on September 28, 2015, as well as peer reviewers for their
constructive feedback on prior drafts of the document.
DISCLAIMER
Certain commercial entities, equipment, or material may be identified in this document in
order to describe a concept adequately. Such identification is not intended to imply
recommendation or endorsement by the National Institute of Standards and Technology, nor
is it intended to im
ply that these entities, materials, or equipment are necessarily the best
available for the purpose.

iv
Table of Contents
Acknowledgments........................................................................................................................... ii
Table of Contents .......................................................................................................................... iv
Executive Summary ........................................................................................................................ v
1 Introduction: Enhancing Safety with Empirically Derived Guidelines for Standardization .. 1
2 Methods for Identifying Critical Use Risk Areas ....................................................................... 2
3 Major Findings from Data Analysis .......................................................................................... 9
4 Methods for Generating Guidelines and Validation Use Cases .............................................. 15
5 Use Cases for Validation Testing to Ensure Safety-Enhanced Design .... Error! Bookmark not
defined.
6 Empirically Based Human Factors Guidance for Safety-Enhanced Design of Health
Information Technology ......................................................................................................... 36
7 Conclusions ............................................................................................................................... 41
8 References ................................................................................................................................. 43

v
Executive Summary
This document provides the empirical rationale for critical patient safety-related usability guidelines
for standardization. As well as requirements for validation testing to ensure safety-enhanced design.
These standardization guidelines are targeted at eliminating ‘never events’ and associated patient
harm by proactively addressing and mitigating the root causes of use errors from EHR design and
implementation elements, as characterized in our framework on the relationship between usability
and patient safety (NISTIR 7804).
Requirements for validation testing are instantiated through realistic use cases that can be applied
during design and evaluation of Electronic Health Record (EHR) systems and for user performance
testing. The ultimate goal is to drive and empower effective and safe human performance in the use
of EHRs. The objective of this research is to enhance safety-related usability with empirically
derived guidance in order to improve the effectiveness and efficiency of EHRs by eliminating or
reducing the most critical and likely causes of patient harm from mistakes and errors in interaction.
This research drew upon five different methods of empirical human performance data collection,
using crosscutting analytic methods, with a diverse set of analysts from different disciplines,
backgrounds, and perspectives. Researchers applied this mixed method approach in order to capture
user expectations, knowledge, and outcomes regarding EHRs. Multiple forms of data were collected
from a variety of user types, allowing for a comprehensive view of EHRs. Two large, multi-hospital
healthcare systems in the U.S. served as sites for most of the data collection, including observations
and interviews. Data collection included: 1) an online survey; 2) site observations; 3) follow-up
interviews with users; 4) usability testing of five different EHRs; and 5) expert reviews of the same
EHRs. Research results demonstrate strong congruence among the data, methods, and the analysts.
Human factors guidelines for standardization, which were explicitly derived from the empirical
evidence obtained through field data collection, are provided to improve the safety-related usability
of EHRs in each of the following three critical use risk areas:
1) Consistently display information critical to patient identification in a reserved area to
avoid wrong patient errors,
2) Provide cues to reduce the risk of entering information and writing orders in the wrong
patient’s chart, and
3) Support efficient and easy identification of inaccurate, outdated, or inappropriate items in
lists of grouped information by having information presented clearly and in a well-organized
manner.
Two use cases, one for the inpatient setting and one for the outpatient setting, are provided for
validation with summative usability testing. Employing use cases oriented to empirically- derived
usability challenges is intended to validate that potential patient safety risks are proactively mitigated
in the tested EHRs. These use cases may also prove useful for organizations for adapting aspects of
the design during implementation and optimization processes to protect against inadvertently
introducing new risks to patients.
vi
Ultimately, this research demonstrates that patient safety is negatively affected when critical safety
tasks are performed with the support of poorly designed EHRs. As a result, mistakes and errors
frequently occur; with end users becoming frustrated and unwilling to trust the systems they are
given and therefore are more likely to rely on potentially unsafe workarounds.

1
1 Introduction: Enhancing Safety with Empirically Derived
Guidelines for Standardization
This document outlines the empirical rationale for critical patient safety requirements instantiated in
use cases that can be used during the design, evaluation, and user performance testing of EHR
systems. Electronic Health Records (EHRs) offer great promise for improving healthcare processes
and outcomes, including increased patient safety. Emerging evidence suggests that the use of health
information technology (HIT) may help address significant challenges related to healthcare delivery
and patient outcomes.
1
For example, three reports suggest that the use of HIT may improve
healthcare outcomes
2
and reduce patient mortality.
3
In addition, the use of HIT is a key component
of a national strategy to improve healthcare quality and patient safety.
4
Given the estimate that one
in three patients will potentially be harmed during a hospitalization,
5
the role for EHRs to improve
patient safety may be significant.
On the other hand, studies found that patient mortality unexpectedly increased following the
introduction of an EHR in a pediatric hospital
6
and that an order-entry system contributed to a severe
medication overdose.
7
Therefore, empirically-derived guidelines for standardization are needed to
foster enhanced ability to protect patients from inadvertent harm from EHRs. As with any HIT, EHR
usability problems that can adversely impact patient safety can be assessed, understood and
managed. Data collected through multiple methods can increase the validity of findings regarding
the magnitude of risk to patients.
The ultimate objective of enhancing safety with empirically derived guidelines for standardization is
to improve the effectiveness and efficiency of EHRs, and thus reduce the opportunity for patient
harm from mistakes and errors. Failing to have effective and efficient EHRs could result in clinical
users ‘extensive workarounds that can directly and negatively impact patient safety.

2
2 Methods for Identifying Critical Use Risk Areas
Researchers applied a multiple research methods approach in order to triangulate user interactions,
experience and dispositions of common encounters with EHRs. Multiple forms of data were
collected from a variety of user types allowing for a comprehensive view of EHRs. Data include: 1)
an online survey; 2) site observations at two geographical locations; 3) interviews with users at these
two locations; 4) usability tests with five different EHRs; 5) and expert reviews of the same EHRs.
A team of researchers with expertise and extensive experience in research methods executed the
effort, aided by three additional researchers, including clinical experts and human factors experts.
Data Collection
Data for this study were collected via NIST Contract Number SB134110CN0107 (UL-Wiklund).
Data collection commenced in September 2010 and concluded in May 2015. Two large, multi-
hospital healthcare systems in the U.S. served as sites for much of the data collection, including the
observations and interviews. Two weeks of observations and 40 interviews occurred in a variety of
care settings and with different types of user groups who routinely used EHRs. There was extensive
effort of unobtrusive ‘in situ’ observation and follow-up interviews in these locations. A total of 86
EHR users were interviewed and observed, including 49 medical assistants and administrative staff
members. Verbatim transcriptions of interviews and researcher field notes provided accurate and
reliable data for the analysis. There were over 300 pages of interview transcripts and 336
observation notations.
In addition, five EHR developers volunteered their EHRs for usability testing. There were a total of
15 two-hour test sessions per EHR, resulting in a total of 63 participants, including 31 providers
(physicians, nurse practitioners, and physician assistants), 21 nurses, and 11 medical assistants.
Several two-person teams, each including a test administrator and a data analyst (i.e., data logger),
conducted the usability tests. All test sessions took place in usability test facilities that included a test
room and adjacent observation room. All test sessions were video recorded. Test data included use
errors, “close calls”, difficulties, anecdotal comments about EHR interactions and quantitative
ratings of the EHR according to a scoring system focused on safety-related usability which was
developed as part of NIST contract SB134110CN0107. This scoring system, using responses as a 5-
point Likert scale from 1 = strongly disagree to 5 = strongly agree, was comprised of these
statements:
• The EHR uses familiar terms, symbols, and units.
• The EHR makes important information stand out.
• The EHR’s workflows match my expectations.
• The EHR makes it easy to detect and correct mistakes.
• The EHR gives me a comprehensive view of a patient’s health.
• The EHR will prevent harmful mistakes.
• The EHR makes it easy to share information with other healthcare professionals.
• I can use the EHR effectively while working under pressure.
• The EHR is easy to learn to use.
• I am confident that I can use the EHR to perform tasks correctly.

3
At the same time, six usability, informatics, and human factors experts independently reviewed the
same five EHRs in order to identify interface strengths and weaknesses of each. Of 665 strengths
and weaknesses identified overall, 60 weaknesses were identified by a human factors expert to
potentially have patient safety implications. Examples include having the patient name displayed on
the lower right corner of the screen, unlabeled graph axes, values displayed without accompanying
units (e.g., 225 without lbs), a value of 11 years and 11 months plotted as 11 years on the X axis of a
graph, not allowing physician users to edit or cancel an order after submission, and requiring one tab
to be open when writing an order and a different tab to be open when submitting a medication order.
Finally, a single academic medical center participated in an online survey, with approximately 2,500
surveys sent to clinicians and administrators from 19 different departments/units. There were 559
responses, of which 339 responses were complete (13.5% response rate). Nurses and physician
providers were the largest categories of user types who responded. There were 21 questions on the
survey, including two open-ended questions: 1) What EHR characteristics make it particularly easy
to use? and 2) What EHR characteristics make it particularly difficult to use?
Data Analysis
Quantitative and quantitative data set/analysis are described in NIST GCR 15-996 “Technical Basis
for User Interface Design of Health IT”.
1
Consecutive qualitative analysis of the interview and
observation data began with multiple readings of the full data set by the lead researcher and one of
the research analysts. Each of these two researchers coded a subset of the qualitative data in order to
begin a conscious and collaborative process of peer debriefing related to coding agreement. The
goal was to insure that the researchers’ use of codes and their application to segments of text was
consistent; “the more coders (using the same codebook) agree on the coding of a text, the more we
can consider the codebook a reliable instrument”
8
(page 310). This process is recommended in
qualitative research in order to establish the “credibility” or “truth value” of the findings.
9,10
During
peer debriefing sessions, researchers operationalized all codes and reviewed the data linked to
various codes. This process occurred regularly during the multiple coding phases, allowing for
continual reflection on and refinement of the codes and their application to the data.
Both researchers continued to read through the interview and observation data, creating tentative
labels for chunks of data that summarized what was emerging from the data. This was the open
coding process
11
or first cycle coding
12
. During this coding cycle, approximately 60 different codes
were used, with 30 of those occurring consistently across the data. While many of the remaining 30
codes only occurred once or twice, several of these represented critical cases where the data seemed
important enough (for example, those related specifically to patient safety). These critical case
codes became part of the code list that was used in the next coding cycle.
Once saturation occurred in the open coding process, the place where no new properties or
dimensions emerged from the coding process, we moved on to axial coding. Axial, or second
cycle
13
, coding provided a means to identify the relationships and connections amongst the open
codes. This allowed for the development of conceptual categories that link the codes and associated
data. Richards and Morse
14
argue that coding “leads you from the data to the idea, and from the idea
1
Available at http://nvlpubs.nist.gov/nistpubs/gcr/2015/NIST.GCR.15-996.pdf. Accessed September 28, 2015.
4
to all the data pertaining to that idea” (page 137). During this phase of the analysis, two top-level
categories of codes: 1) issues related to input and/or handling of data and information and 2) issues
related to understanding and use of the EHRs were identified.
Finally, selective coding identified core variables and emergent themes that occurred across the data
set.
15
Each researcher developed and shared memos and models about ongoing interpretations of the
data as a means to identify conceptual categories and move toward the development of emergent
themes for critical use risk areas that allowed researchers to predict patterns “of what may be
observed and what may happen in similar present and future contexts.”
16
Here, three major critical
use risk areas emerged as our ultimate findings: Identification of information, Consistency of
information, and Integrity of information.
At the same time, the lead researcher and the data analyst coded the usability test data. The same
conceptual categories and emergent themes developed in this data as in the interview and
observation data. Similarly, the lead researcher reviewed the survey data for overlap between this
and other data sources. Again, similar ideas surfaced across the data sets. Finally, the human factors
researcher examined expert reviews to discern patterns across reviews related to the issues under
consideration, specifically the relationship between the EHRs and patient safety. The lead
researcher used the findings to map back to the other data forms. The conceptual categories and
emergent themes are represented across the data sets, demonstrating the strength of the findings.
Examples of Codes, Categories, and Critical Use Risk Areas
In qualitative research, a code “symbolically assigns a summative, salient, essence-capturing,
and/or evocative attribute for a portion of language-based or visual data.”
17
Coding is a cyclical act
that serves as an intermediary between data collection and data analysis. Saldaña
18
argues that
qualitative codes capture essential elements of the data, and when those elements form clusters they
can “facilitate the development of categories and thus analysis of their connections” (p. 8). Codes
are rooted in the data, but as coding and analysis continue, codes and categories become more
refined, and often more conceptual and abstract. A further shift is evidenced “when the major
categories are compared with each other and consolidated in various ways, you begin to transcend
the “reality” of your data and progress toward the thematic, conceptual, and theoretical” (p. 12).
Below are excerpts of particular pieces of interview data and the codes applied to them, followed by
how these led to broader categories of analysis and later to emergent themes that ran across data sets.
It should be noted that the excerpts below are exemplars to demonstrate how data were coded,
however many more data segments were coded with the same codes. Many codes resurfaced
multiple times in the same interview and most occurred across all interviews.

5
Table 1. Examples of individual data excerpts and codes
DATA CODE(S)
“Sometimes, I might issue a rapid strep test and then save the note as a draft so that I have to go back in at end of day to save as
final based on strep test results. I might need to edit [the] plan, and then I also give patient both plans of action. [The] system will
send me a message reminding me to save the drafts, but you have to be paying attention, and there are a lot of things to pay
attention to”.
DRAFT VS. FINAL;
RELIANCE ON
MEMORY
“Running through a list of med[ication]s can take quite a bit of time. When a patient gets admitted to the hospital and discharged,
the med[ication] list changes. To me, there is a right way to write a prescription, so that we can communicate it. When [a] patient
gets discharged, sometimes pertinent medic[ations] can get deleted, and the format changes. When they get discharged, the units
might be off, the units might say mg, but the mom tells me she gives mL. The mom won’t know what mg means. If [the] patient
come[s] from [the] hospital, it might take me a half hour to update it”.
MEDICATION LISTS
CHANGE;
MEDICATIONS
DELETED;
UNITS OF MEASURE
CHANGE
“I think you could send a message on the wrong patient. Let’s say that the mom called and the child has breathing difficulty and
you are accidentally in [the] wrong record. It’s not the information that gets into the wrong patient, it’s knowing what patient the
information belonged to. Sometimes, [the] wrong vaccine gets recorded. I notice something might be wrong, the age is wrong, I
can get someone to go in and delete [the] vaccine, but then we are missing the information on [the] proper patient’s record. We
may be able to identify later when that patient comes in, but if we can’t find it, the patient gets an extra vaccine”.
WRONG
PATIENT/CHART;
VACCINE ERRORS
“My patient list is incorrect. It is not a complete patient list and I don’t know why. Sometime over the past 6 to 8 months 2/3 of
my list got purged. I have to remember the patients’ names and search through [the current EHR] to find…It is very frustrating
because I have no idea why it happened. Suddenly, one day I had 3,200 patients on my list and the next day I had 700. It doesn’t
make any sense. Every day the system does not feel firm or complete”.
WRONG PATIENT
LISTS;
FRUSTRATION
“A patient going from outpatient to inpatient or vice versa. Often times the medications are not addressed appropriately at those
transition periods. Often what’s in the discharge summary is not what’s in the medication list in the patient summary and so often
times it’s confusing to figure out. The person discharging the person is not diligent in updating the medications and I don’t know
if this happens, but it seems to be that somehow the inpatient medications and discharge summary medications should all auto-
populate”.
WRONG/DISCREPANT
MEDICATION LIST;
NEED FOR AUTO-
POPULATION
“No checks and balances for diagnoses in patient summary. Say a patient is seen by one provider and provider goes in patient
summary, sees that they have [a] scar on [the] chest so must have had CAD [Coronary Artery Disease] and surgery. If I see the
patient and change the summary all around and correct it, say they never had a heart attack, say I update that, if that patient goes to
see someone else… there’s no accountability. Anyone can change anyone else’s patient summary. Patient could come back to me
after seeing 3 other people, no longer looks like what I spent an hour updating. I can go back and look at my patient summary and
try to paste it forward. But [there] are oftentimes disease-specific information that other services might delete, and they delete it,
but it’s actually the record. Can be frustrating and lead to errors”.
CHANGES MADE TO
NOTES;
NO
ACCOUNTABILITY;
DELETED
INFORMATION;
FRUSTRATION;
ERRORS
6
Table 1. Examples of individual data excerpts and codes (Cont.)
DATA CODE(S)
“Patients can receive 2 doses of medication because of how read-only scripts are handled in the system, e.g., [for example] read-
only means that there is no physical order, the pharmacy can view and dispense the medication, but with a read-only order there is
no way to scan or manually document that the patient received the medication. Order could be filled and given twice. EHR user
has to complete 8-9 clicks to get to a more detailed view to see comments if the script has been given to the patient”.
WRONG
MEDICATION OR
DOSE;
DIFFICULTY OF USE
(8—9 CLICKS)
“I’ve seen this EHR [at this hospital] go from a reporting mechanism to a data entry mechanism, to the point where it becomes a
file cabinet that you shove paper into. I guess if you control it [data entry], you know where things are. But, if my assistant or my
colleagues begin to use my file cabinet, pretty soon I’m not going to know what’s in there. I might be able to find a paper I filed 6
months ago, but it’s a needle in a haystack. Indexing is not standardized. It’s difficult to figure out where to start. [This is] what
am I worried about”.
“FILE CABINET”;
OUT OF CONTROL;
“NEEDLE IN
HAYSTACK”;
NEED FOR
STANDARDIZATION
“The list in the EHR is populated by multiple individuals. It’s a mish mash. Stuffing information in drawer, I may own a section
of that, not [the] entire piece”.
“MISH MASH” OF
INFORMATION
USED BY DIFFERENT
INDIVIDUALS;
POSSBILITY FOR
CHANGES/ERRORS
“Let’s say the patient is on Coumadin and then an internist gives an antibiotic. If [I] get prompted to refill the Coumadin, [then] I
get prompted that [the] patient is on an antibiotic and it tells me to consider decreasing [the] dose. That’s a robust decision support
piece that only works with providers in this EHR system [at this hospital]. It only works if I’m here and I see that you prescribed
that. It [EHR] doesn’t reflect the antibiotic received at [the] walk-in clinic”.
WRONG
MEDICATION OR
DOSE;
MEDICATION
INTERACTIONS
“Omitted information. It would be through omission, or you chart on the wrong kid. That would be human error. Safety thing is
when patient was omitted and all information was left out. The log in/log out thing is a huge pain in the butt. If I’m working at the
desk and someone says “Hey,” I run. If User Y comes back and was working at that spot, he might sit down and chart on me [the
chart I was working on before leaving]”.
OMITTED
INFORMATION;
WRONG
PATIENT/CHART
7
As coding continued, codes seemed to cluster into two major conceptual categories: 1) input and
handling issues and 2) understanding and use issues. For example, “Draft vs. Final” seemed to
be an input issue, as did “Changes Made to Notes” and “File Cabinet.” These codes were
connected by their relationship to the ways in which data made its way (or not) into the system.
Likewise, data related to “Medications Change” or “Wrong Patient” clustered around the ways in
which participants understood and used the EHRs. Sometimes chunks of data related to both
categories, as in the case of “Wrong Patient/Chart.” For example, P43 above noted that someone
might be working on a chart, need to leave for another task, and then someone else would begin
to work on it, thinking it was a different chart. This was an input issue (in that data was input
into the wrong chart), but also a use issue in that it was often difficult to discern which chart one
was in at a given time. The second cycle of coding allowed analysts to revisit previously coded
data and cluster it around these two conceptual categories. During this process, analysts noted
that both categories produced issues related to Identification of Information, Consistency of
Information, and Integrity of Information. These critical use risk areas pulled together a variety
of related codes that were united conceptually. For example, Identification of Information
represented those instances in the data where a piece of information was unable to be identified,
was misidentified, or was difficult to identify (this could be a patient name, a medication, a chart
number, or whether something was a draft versus a final entry). Consistency of Information
related to where and how information was presented, and often referred to a lack of
standardization in where and how information was presented as in where and how the patient
name was presented or a medication was entered. Finally, Integrity of Information encompassed
those codes where the accuracy of information was difficult to discern, sometimes due to
information being changed, being deleted, or not being entered.
Once coding of observation and interview data was complete, researchers looked across data sets
for congruence of analysis. Many of the codes generated in the analysis of observation and
interview data also emerged in the usability tests and expert reviews. For example, location of
patient name, unlabeled graph axes, values displayed without accompanying units, not allowing
physician users to edit or cancel an order after submission, and requiring one tab to be open
when writing a medication order and a different tab to be open when submitting a medication
order. Survey data also corroborated the coding structure and the subsequent development of
conceptual categories and themes. Identification of information, Consistency of information, and
Integrity of information cut across the data as major areas of use risk.
Trustworthiness
According to Lincoln and Guba
9
, trustworthiness involves establishing credibility,
transferability, dependability, and confirmability. Triangulation is one way to insure a
comprehensive, well developed, and systematic analysis that provides for credibility in the
process and the findings.
19,20
Triangulation can take many forms, including triangulation of
methods (using multiple methods for both data collection and analysis), triangulation of sources
(from within the same method—for example having Medical Assistants, Nurses, and Providers
as participants in the interviews and usability tests), and triangulation of analysts (to provide for
differing analytic lenses and perspectives). Researchers in this project used all three types of
triangulation to provide a more robust process and insure a more holistic and comprehensive
picture of the findings. Mays and Pope
21
suggest additional mechanisms for enhancing the
8
trustworthiness of a study, including respondent validation, where study participants are asked to
respond to and assess the researchers’ interpretations. While traditional respondent validation
(or member checking as it is also known) was not utilized here, researchers held a debriefing
session with people from a range of roles and positions, including nurses, doctors, and human
factors experts in order to obtain feedback regarding the analysis, interpretation, and findings.
Peer debriefing and respondent validation provided additional credibility for the study.
9
The use of “thick description”
9
and the voices of participants allow for greater transferability, or
the ability of readers to determine for themselves whether or not the results generalize to their
own situations. The presentation of extensive quotes and the detailed description of the coding
and analysis process in this report allow for such transferability. Dependability refers to how
likely it is that the findings would be consistent if the study were done again with a similar set of
participants in a similar context. Dependability can be achieved through the use of an external
audit where researchers who were not involved in the project review the process and products of
the research. In this study, the debriefing session with a variety of different experts offered a
space for presentation and discussion of the research process and the findings. Confirmability
provides a mechanism to determine if the conclusions, recommendations, and/or interpretations
can be traced to their sources, insuring that the findings are a product of the study and not of
researcher bias. An audit trail of the data and its processing allows for such confirmability.
Mays and Pope
20
also argue that a clear presentation of the data collection and analysis methods
provide for greater validity of the study.

9
3 Major Findings from Data Analysis
This research examined the use of EHRs in different healthcare settings and with different types
of users in order to gain a comprehensive view of the EHR impact. The objective is to improve
their effectiveness and efficiency and thus reduce the likelihood of contributors to avoidable
patient harm. We found three overarching themes representing critical areas of use risk, based
upon a convergence of triangulated evidence from all of the data sources: identification of
information, consistency of information and integrity of information. Within each overarching
risk area are subcategories, characterized by prototypical statements and questions, and possible
consequences, all rooted in the data. These are detailed in Table 2 below. Across all three of the
risk areas and their related subcategories there arose several major issues related to patient
safety: 1) the occurrence of unintended actions; 2) the likelihood of use errors; and 3) the high
level of user frustration. The three areas and their related issues highlight a lack of effectiveness
and efficiency related to EHRs. Ultimately, both the objective (actual observation and analysis
of user performance) and subjective data demonstrate that these issues negatively affected patient
safety during safety-critical tasks and times. For example, one participant discussed transition
periods and how these often led to discrepancies in medication lists:
“So the patient going from outpatient to inpatient, or inpatient to outpatient. Often times
the medications are not addressed appropriately at those transition periods, and so often
times what's in the discharge summary is not what's in the medication list in the patient
summary...And so often times it's confusing to figure out…The patient can end up being
confused and taking either too much or too little, or the wrong medication combination.
I, as the provider, on the other hand am unclear on what the patient is actually taking,
and it leads to confusion when the patient calls and says, "I'm not responding to the
treatment in the hospital. Then I have to go back and try to figure out, okay, are they not
responding because they're not actually taking the right medicine, or something like that?
And it also leads to confusion because the-- I had one patient who called our office from
their hospital bed and said, "They're sending me home. I'm confused about my
medication and nobody will talk to me." So not only was the documentation fraught with
errors in instruction to the patient, they were just as confused as I was trying to figure out
what they were going home with.”
The data excerpt above demonstrates how the integrity of the information is compromised
leading to incorrect dosages or medication combinations. Effectiveness is diminished as the
likelihood for critical use errors increases and efficiency is affected since it will now take
additional time to identify accurate information. This relationship was seen many times across
the data set. Also related to integrity of information, a different participant noted how difficult it
was to create an accurate patient summary:
“Actually, I was in with a patient. Gosh, was it Monday? I was trying to update the
patient summary because that's essentially what I spend a lot of my time doing now with
all new patients is I'm building all the patient summaries. Let's see if I can get to this
patient summary. What ended up happening is, as I'm updating, I can hit update here,
and when I'm updating, I can't see labs, I can't see anything else. I'm asking them,
"When's your last tetanus? Have you had your diabetes screen checked?" And I can go
up here to Actions, which I've now learned, and I can open up any one of these things in
a different-- let's see if we can get the labs. I can open up labs, but what happened to me
10
last time was that I was trying to open these up and it overwrote whatever I was doing
here. It wouldn't let me save anything. It wouldn't let me get back to it to save it.”
Not being able to see lab results and other pertinent information, as well as not being able to save
information as needed also reduce effectiveness and efficiency and create a situation where
frustration and unintended actions are likely to occur.
In addition to the integrity of information, the consistency of information presentation
and where to find it was a common issue. Two other participants articulated examples that many
others corroborated related to this pattern:
“I’ve seen this EHR here at [hospital] go from a reporting mechanism to a data entry
mechanism, to the point where it becomes a file cabinet that you shove paper into. I guess
if you control it, you know where things are. But, if my assistant or my colleagues begin
to use my file cabinet, pretty soon I’m not going to know what’s in there. I might be able
to find a paper I filed 6 months ago, but it’s a needle in a haystack. Indexing is not
standardized. It’s difficult to figure out where to start…
Because if you read through it and you don't change it to make it up to date, and you
don't bring forward the information that you've learned - they've got a new allergy, or
they used a medicine that you gave last time and they have an adverse affect, or anything
that they've told you that happened since you last used that note. If you don't bring it in to
that note, and you don't record it, then not only have you created a safety concern for
that patient, you've created a liability for yourself and for the institution.”
Finally, the identification of information arose as a major issue, with many participants
noting how difficult it was to easily locate and identify information and how easy it was to be in
the wrong place. The data excerpt from a different participant below clearly illustrates the
potential consequences of this issue:
“An example today: When I went in today to see a patient, there were two notes saved,
one was a 3 year old draft that my nurse started, the other note was for a different
patient. That’s easily solved. I went in the room, noticed an incorrect note. I sent a
message to the nurses. Asked them to delete it from record. But, in the meantime, one of
my staff members went into room of 12 month old and couldn’t find the record. I think
you could send a message on the wrong patient. Let’s say that the mom called and the
child had breathing difficulty and you are accidentally in wrong record. It’s not the
information that gets into the wrong patient, it’s knowing what patient the information
belonged to. Sometimes, [the] wrong vaccine gets recorded. I notice something might be
wrong, the age is wrong, I can get someone to go in and delete the vaccine, but then we
are missing the information on the proper patient’s record. We may be able to identify
later when that patient comes in, but if we can’t find it, the patient gets an extra vaccine.”
It is important to note that the examples presented above serve as exemplars for a broad range of
data found across the different methods that support the use risk areas and subcategories. These
are by no means unique statements, but representative of the data as a whole.

11
Table 2. Summary of Analytic Findings on Major Safety-Related Risk Areas and Possible Consequences
Areas of Critical Use Risk
Subcategories
Possible Consequences
Identification of Information
Am I in the right place and doing the right
thing?
• For patient
• For patient lists
Incorrect patient list
Who are these patients?
• Wrong treatment
• Wrong billing
•
Wrong charting of information
• Missed, omitted, delayed care
• Care or billing activity conducted on the wrong patient
• Have to pull up every patient chart
• Wrong medication ordered
• For records
• For medication/order
Passing/sharing information
What happens in the handoff?
Multiple EHRs used
What happens when EHRs don’t coordinate?
• Data/information are not recorded in EHR
• Misrecording or recording in wrong patient chart
Fragmented information
Data are often fragmented and found in multiple
places
• Often no context for displayed information
Consistency of Information
Why are things not listed and displayed in
standardized ways?
Misidentified patient/chart Where am I?
Record number is incorrect/Patient name is
misidentified.
• Documentation/orders in wrong chart (often without
knowing it)
• For information
• For organization
• For format
• For different systems
• For draft vs. final versions
• For omissions and/or changes
Supplements used
Did I remember to transfer data to the EHR?
Paper, whiteboards frequently used (reliance on
memory)
Multiple EHRs used
Where do I find X on this EHR?
Functions and screens shift Where is my
information?
• Cannot find information when needed in the EHR
• Reliance on memory for transfer of information/data
Cannot find information
Where is my information? Am I in the right
place?
• On screen
• In file
• In EHR
• Functions and screens shift
• Information found in different places (including record
number, patient name, medications prescribed, etc.)
Standardization of where things are and what
they are
• Location and format of date
• Location of record number
• Location and format of name
• Format of amount (e.g., metric vs. US)
• Running list of current medications
• Notation in wrong record
• Incorrect diagnosis or prescription
• Incorrect medication or order OR double vaccine

12
Table 2 Summary of Analytic Findings on Major Safety-Related Risk Areas and Possible Consequences (Cont.)
Areas of Critical Use Risk
Subcategories
Possible Consequences
Integrity of Information
Why and how are things changed, deleted,
or omitted?
• Lack of control over changes in dates,
notes, units of measure
• Inability to know what information is
Cannot figure out EHRs
How do I do this?
• Navigation is difficult
• Adding/deleting data is difficult
• Scrolling through long notes is time-
consuming
• More likely to just use whiteboard/paper and not put
data in EHR, resulting in incomplete files/charts
valid, relevant, and up to date
Draft vs. final version
Is this a draft or final version? Often forget to
finish a final version
• Omissions of data/information; notation of incorrect
data/information
•
What happens if change in patient condition in interim?
Changes to note/chart
You changed what?!!
• Different user can change someone else’s
note/input
• Information lost
• Inaccurate and/or incomplete data and charts
Common references not there
Why are height and weight not here? (and other
common data like vital signs)
• Having to do things (input) multiple times or search
multiple places
13
Included in the two use cases are the following aspects, categorized by the areas of use risk that
emerged from the data analysis and related to supporting evidence from the data analysis:
1) Critical Use Risk Area 1: Identification of Information
A) Accidentally transposing a patient’s first and last name is easy to do when the
names are both commonly used first names as well as possible last names
(e.g., William John, John William). This increases the potential for making
clinical orders or documenting in the wrong patient’s chart due to the ease of
inverting the names when searching for the chart, flipping the open chart to
another person and mistakes can more easily occur when quickly scanning the
name to confirm that the right chart is open. In the use cases for eligible
providers and nurses, both William John and John William need to be
included in the patient list.
B) Getting confused as to which chart is actively open for ordering medications
and viewing information is challenging when there is an interruption in the
midst of providing care for one patient in order to a high priority activity like
look up the current medications for another patient in response to a phone call
from the Emergency Department nurse for a patient who is not able to provide
the information reliably.
C) Identifying an allergy to the common sugar substitute that is contained in the
hospital’s standard diabetic diet is challenging when relying upon clinical
decision support alerts that are not designed to cover this scenario and/or have
high false alarm rates.
D) Being interrupted while providing care to one patient can increase the risks of
performing clinical actions or documenting information in the wrong patient
chart.
2) Critical Use Risk Area 2: Consistency of Information
A) Having a primary care provider in the outpatient setting identify that the
results of a diagnostic (MRI imaging) test are not available because they were
not ordered as planned during a prior hospital stay can be challenging when
results from within an organization and from other organizations are not
displayed and sorted in a consistent fashion.
B) Managing and documenting an allergy to a preservative in intramuscular
vaccines, thimerosal, is challenging because it differs from how the typical
allergy to a medication is identified and alerted with clinical decision support
and visualization paradigms Clinical decision support recommends ordering a
vaccination for influenza despite the patient having an allergy to thimerosol,
which is a preservative in the vaccination in the traditional injection delivery
mechanism. A different form of the vaccine (that does not contain thimerosol)
needs to be ordered to avoid an allergic reaction.

14
C) Treating an infectious eye disease requires coordinating care with other
specialized personnel, including infectious disease specialists and eye care
specialists. It can be particularly challenging to coordinate care using “read-
only” documentation.
2
D) As soon as the nurse notices that the patient had a markedly pink irritated right
eye on morning rounds, this information is critical to share quickly with other
care providers in order to protect healthcare workers and other patients from
infection by initiating and maintaining contact isolation precaution
procedures. Sharing this information across transitions of care is similarly
important.
3) Critical Use Risk Area 3: Integrity of Information
A) Managing medications requires reviewing medication lists which have
discrepancies.
3
B) Reviewing the laboratory results of a blood test cannot be done during the
primary care provider outpatient clinic visit with the patient because the
results are not available for review.
C) An imaging test that was not completed in the acute care setting is not readily
discoverable during the follow-up visit with the primary care provider as it
was not completed in the primary care setting.
2
Supporting evidence from the interview data: “Patients can receive 2 doses of medication because of how read-only scripts are
handled in the system (e.g., read-only means that there is no physical order, the pharmacy can view and dispense the medication,
but with a read-only order there is no way to scan or manually document that the patient received the medication. Order could
be filled and given twice. EHR [Electronic Health Record] user has to complete 8-9 clicks to get to a more detailed view to see
comments if the script has been given to the patient.”
3
Supporting evidence from the interview data: “I guess part of the biggest thing that we noticed, or that I see, is the transition
periods. So the patient going from outpatient to inpatient, or inpatient to outpatient. Often times the medications are not
addressed appropriately at those transition periods, and so often times what's in the discharge summary is not what's in the
medication list in the patient summary... And so often times it's confusing to figure out. The person discharging the patient is not
diligent in updating the medications. And I don't know if this happens but it seems to me somehow the inpatient medications and
discharge summary medications should all populate the updated patient summary, but I don't know if that happens. And so if
there's a discrepancy between what's in the patient summary med-list versus what's in the discharge summary, what can happen
as a result of that? The patient can end up being confused and taking either too much or too little, or the wrong medication
combination.”

15
4 Methods for Generating Guidelines and Validation Use Cases
Group of the human factors experts collaboratively mapped the findings from the data analysis to
human factors terminology in order to relate the insights to what is known in the human factors
field about contributors and barriers to successful, high reliability, and high reliance performance
by experts in domains with high consequences for failure. This translation resulted in
transforming the major findings into human factors issues and deficiencies, which enabled a
more targeted search for existing solutions and standards on which to base the recommendations.
Subsequently, a team composed of a methodologist, clinical physicians, clinical nurses and
human factors experts provided guidance on the generation of the recommendations and use case
during a focused two-day working meeting. As a result of this meeting, the team generated
safety-related usability technical guidance that draws upon existing human factors knowledge
and is empirically grounded and prioritized on the basis of being repeatedly raised as important
across five data collection methodologies.

16
5 Use Cases for Validation Testing to Ensure Safety-Enhanced
Design
The research findings provide empirical evidence about critically important usability issues that
could potentially have negative impacts on patient safety for providing clinical care with the
support of EHRs in both the inpatient and outpatient care settings. These issues provide the
foundation for the creation of two challenging use cases intended for summative usability testing
validation.
Healthcare is delivered within a system encompassing both ambulatory and inpatient settings. As
such, designing support for clinical care in either or both of these settings is challenging even for
an ordinary evolution of the care of a typical patient over a select time period in his or her life
that requires continuity of care across multiple providers with dedicated roles.
In this section, we provide for evaluation purposes one use case for inpatient care and one use
case for outpatient care. These two use cases are contextualized within an overarching narrative
for a single patient with multiple care activities conducted by multiple types of care providers.
When recruiting study participants for the validation testing, there are two categories of care
providers, 1) eligible professionals (medical doctors, nurse practitioners, or physician assistants)
and 2) nurses (registered nurses, licensed practical nurses). By employing the same patient for
the validation testing, it is possible to reuse demographic information and test data.
Overview of both use cases
The two use cases are situated within an integrated series of care encounters, consisting of:
1. An acute care hospital admission through the emergency department of a 45-bed community
hospital for a number of concerning symptoms, including chest pain and a productive cough.
2. An outpatient visit with a primary care provider two years later, after a recent hospital
admission for a possible stroke
17
The use cases for evaluation cover selected aspects of the interactions dependent on the
electronic health record. Initially, an overall scenario of the patient visit is provided. Next, the
detailed steps involved by each user interacting with the EHR are enlisted. This is followed by a
short description of the critical usability issues in the tasks of each of the user roles.
Use Case 1: First Hospital Stay
We discuss the use case in several parts. The complex scenario is likewise broken into relevant
parts for better understanding and application. The scenario description is followed by the user
tasks based on roles and the workflow per the scenario. Hence, the user may appear repeatedly as
called by the events mentioned in the scenario. We associate the critical usability issues
encountered in the performance of the tasks under each role as a subcategory.
Scenario 1, Part I
Mr. William John is a 65-year-old Hispanic male who presents to the Community General
Hospital Emergency Department with complaints of severe chest pain, difficulty breathing and
productive cough. Mr. John has a known history of Type 2 diabetes mellitus and
hypercholesterolemia. His allergies include Thiomerisol and “pink sweetener”. He is triaged and
taken into the Emergency Department (ED). The ED nurse records the vital signs, which are
within the normal limits except for lower oxygen saturation of 90% and an increased heart rate
of 110 beats per minute, and informs the Emergency Physician. The Emergency Physician orders
oxygen therapy per nasal cannula immediately, 12 lead EKG, serial troponin levels, chest X-ray,
sputum gram stain now, CBC, continuous telemetry monitoring, finger stick blood glucose
following the hospitals s diabetic protocol and continuation on his routine medications of a long
acting insulin, regular insulin on a sliding scale, atorvastatin, vitamins and aspirin. He also starts
the patient on azithromycin. He orders an 1800 calorie diabetic diet. The X-ray is confirmatory
for pneumonia. The first troponin is negative. An initial 12 lead EKG reveals abnormal but non-
significant ST segment changes. There is no cardiologist available and the internist will be the
admitting physician.
Scenario 1, Part II
Mr. John is admitted to a Medical-Surgical (Med-Surg) unit under the care of the internist
(admitting physician) for observation and treatment. Vital signs including O
2
saturation had
returned to normal. The resident physician informs the attending physician about the condition
of the patient. The nurse collects the specimens and sends them to the lab in a labeled container.
The attending physician, during rounds, changes the O
2
therapy to “as needed” to maintain
oxygen saturation above 96%.
Scenario 1 Part III
Day 2: The nurse, when assessing the patient in the beginning of the shift, notices that the patient
had a markedly pink itchy irritated right eye with a tearing sensation. The patient reported that
18
he was on some eye drops in the distant past, but did not recall the name of the medication. The
doctor who was then providing eye care moved out of town, and he does not remember the
clinic’s number.
The nurse had a high suspicion of viral conjunctivitis and puts the patient in contact isolation.
She asked the physician if he wanted an Ophthalmology consult. Per the physician order, she
requested the consultant Ophthalmologist. The ophthalmologist, during the consult, was able to
elicit a history of being in contact with a family member that recently had “pink eyes”. The
patient was an occasional contact lens wearer but had none recently. The ophthalmologist
established that the visual acuity, intraocular pressure, and ophthalmic exam were normal except
for signs and symptoms consistent with viral conjunctivitis. The ophthalmologist ordered topical
tetracaine 1% to be applied by the ophthalmologist to both eyes (and to have the bottles available
in the patient’s medication tray for when she rounded on the patient). He ordered that the patient
be able to self-administer preservative free artificial tears in single-use vials prn (as needed).
Because of excessive discharge, she also ordered that an assay for adenovirus be available on the
patient’s floor. The ophthalmologist planned to return the following day or ask the patient to
come to follow up in the office in 24 hours should the patient be discharged.
Scenario 1, Part IV
Day 3: The troponin levels remained negative, and there was no change in the EKG. Mr. John
had decreased chest pain and cough and other vital signs are normal. The patient stabilizes in 48
hours with the lab report positive for growth of streptococcus pneumoniae and confirming
sensitivity to azithromycin. The blood cultures returned negative with no growth. He is
discharged home with a diagnosis of pneumonia and conjunctivitis to follow up as an outpatient
in seven days with his primary care physician. He is asked to see the ophthalmologist the next
day to follow up on his viral conjunctivitis since he left the hospital before seeing him. At
discharge, the nurse hands over to the patient the summary with the discharge instructions.

19
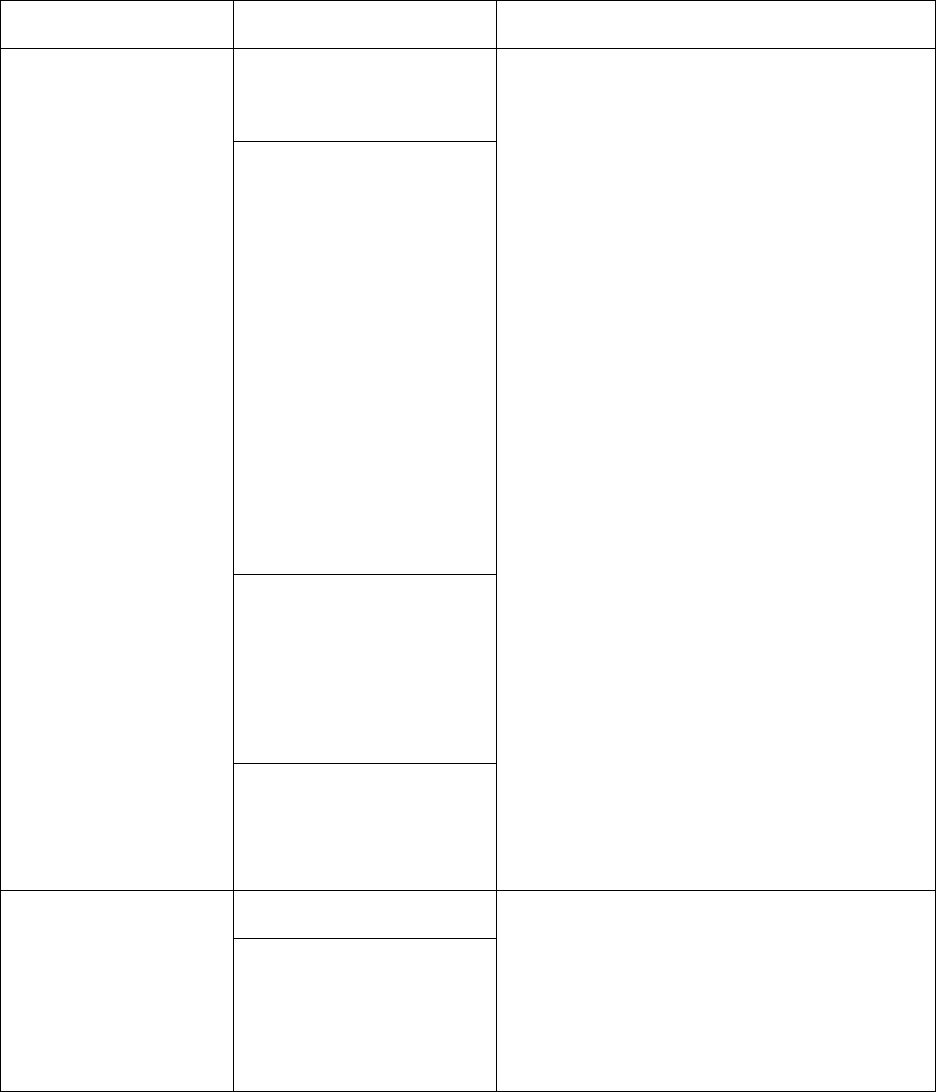
Figure 1. Sequence of events in first hospital stay included in validation testing
20
Use Case 2: Outpatient care after second hospitalization
Scenario 2, Part I
Mr. John is now a 67-year-old male who presents to the Community General Hospital
Emergency Department with complaints of headache, and a reported two short periods of
confusion. He has just recovered from influenza that kept him bedridden at home for 8 days with
vomiting and diarrhea. Mr. John is a known patient of Type 2 diabetes mellitus and
hypercholesterolemia. The patient is triaged and taken into the Emergency Department. The ER
nurse records the vital signs, which are within the normal limits. The Emergency physician
orders electrolytes, CBC, a chest x-ray, CT scan, EKG, echo cardiogram, carotid artery Doppler
and calls the internist who admits the patient to the ICU for evaluation of a possible stroke or
TIA and orders an MRI. The MRI in the hospital is out of order and the MRI is not done. The
echocardiogram results are scanned into the chart in the media section instead of cardiology
where they are usually located. All other tests are negative except the lab tests come back with a
low sodium and potassium and this is resolved within 24 hours by intravenous fluids. He
receives orders for an MRI outpatient, Coumadin therapy for anticoagulation and teaching by the
pharmacist.
Mr. John is sent home with a diagnosis of possible transient ischemic attack (TIA) and discharge
instructions to follow up as an outpatient in seven days with his primary care physician and in
three days with a neurologist. He receives five prescriptions to fill immediately.
Scenario 2, Part II
Upon coming into the office of his primary care physician on day two after discharge, Mr. John
reports he feels much better but still gets headaches. The primary care doctor looks for the tests
done at the hospital. He sees the MRI and echocardiogram were ordered but cannot find the
results. The physician gets several calls during the outpatient encounter from the emergency
department where another of his patients, Bill Bates, has arrived with chest pain so he stops and
takes the urgent call. After addressing the needs of Mr. Bates, lab tests are drawn and Mr. John is
sent home and will see the neurologist in the morning.
The urgent call is about Mr. Bill Bates. This interruption starts with the nurse in the primary care
physician’s office being called to the phone. The emergency department nurse says that Mr.
Bates has come to the ED with a severe nosebleed and headache. The emergency department
needs to know if Mr. Bates is on Coumadin. Mr. Bates cannot remember his medications and left
them at home.

21
Figure 2. Sequence of events from second hospital day which are reviewed during the outpatient
visit during validation testing
22
The findings from the data analysis have implications for the design of use cases for ensuring
safety-enhanced design in the context of these activities, in addition to others:
1. Ordering medications
2. Ordering laboratory tests
3. Ordering diagnostic imaging tests
4. Avoiding drug-drug, drug-allergy, and food-allergy interactions
5. Maintaining the problem list
6. Maintaining and reconciling the medication list
7. Maintaining the medication allergy list
8. Interpreting the recommendations from clinical decision support
9. Using the electronic medication administration record
10. Performing clinical information reconciliation and incorporation
11. Electronic prescribing of medications
When conducting summative usability testing evaluations, representative, appropriately licensed,
participants simulate the roles of user categories (e.g., eligible professionals and nurses). The
mapping of the listed activities above and the user category roles are:
1. Eligible professional (Medical Doctor, Nurse Practitioner, or Physician Assistant) role
a. Computerized provider order entry – medications
b. Computerized provider order entry – laboratory
c. Computerized provider order entry – diagnostic imaging
d. Clinical decision support
e. Drug-drug, drug-allergy interaction checks
f. Problem list
g. Medication allergy list
h. Medication list
i. Clinical information reconciliation and incorporation
2. Nurse role
a. Electronic medication administration record
b. Vital signs documentation
c. Clinical decision support
d. Drug-drug, drug-allergy interaction checks
e. Medication allergy list
f. Clinical information reconciliation and incorporation
g. Retrieve imaging results

23
Table 3: Usability Test Tasks for Safety-Enhanced Design (Representative Use Cases)
Use Case 1: First Hospital Stay
Scenario 1, Part I: Triage Nurse
Participant is now logged in as the Triage Nurse
Critical Task
Scenario Information
Usability Test Task
Patient chart has been
“initiated”
Nurse documents patient’s
demographics
Patient = Mr. William John
Age = 65 years
Ethnicity = Hispanic
Sex = Male
• Sign on to the System
• Open the patient record for Mr. William John
• Enter the provided demographic information
for this patient into the System
Nurse enters patient’s
complaints, current
illnesses/conditions (history),
and allergies
Patient complaints = severe
chest pain, difficulty
breathing, and productive
cough
Enter the provided clinical information for this
patient into his patient record
Current illnesses/conditions
(history) = Type 2 diabetes
mellitus,
Hypercholesterolemia
Allergies = thimerosal and
“pink sweetener”
Nurse documents triage
information with disposition
to Emergency Department
(ED)
Patient is triaged and taken to
the ED
Enter information into the patient’s record about
triaging and transporting him to the ED

24
Scenario 1, Part I: Emergency Department Nurse
Participant is now logged in as the ED Nurse
Critical Task
Scenario Information
Usability Test Task
ED nurse verifies
information documented
by the Triage nurse
Patient = Mr. William John
Age = 65 years
Ethnicity = Hispanic
Sex = Male
• Sign on to the System
• Open the record for Mr. William John
• Review the provided demographic and clinical
information that were entered into his record
by the Triage nurse
Patient complaints = severe
chest pain, difficulty
breathing, and productive
cough
Current illnesses/conditions
(history) = Type 2 diabetes
mellitus,
Hypercholesterolemia
Allergies = thimerosal and
“pink sweetener”
ED nurse records the
patient’s vital signs, and
notifies the ED physician
Temperature, Blood Pressure,
Respiratory Rate = within
normal limits for an adult
male
• Enter the provided clinical information for this
patient into his record
• Enter a note stating that the ED physician was
notified about the increased heart rate and low
O
2
Saturation
Heart rate = 110 BPM
O
2
Saturation = 90%

25
Scenario 1, Part I: Emergency Physician
Participant is now logged in as the ED Physician
Critical Task
Scenario Information
Usability Test Task
ED physician verifies
information documented
by the Triage and ED
nurses
Patient = Mr. William John
Age = 65 years
Ethnicity = Hispanic
Sex = Male
• Sign on to the System
• Open the record for Mr. William John
• Review the provided demographic and clinical
information that were entered into the record
for this patient by the Triage and ED nurses
Patient complaints = severe
chest pain, difficulty
breathing, and productive
cough
Current illnesses/conditions
(history) = Type 2 diabetes
mellitus,
hypercholesterolemia
Allergies = thimerosal and
“pink sweetener”
Temperature, Blood Pressure,
Respiratory Rate = within
normal limits for an adult
male
Heart rate = 110 BPM
O
2
Saturation = 90%
ED physician orders O
2
therapy, 12-lead EKG, lab
tests, a radiology test,
telemetry, medications,
and diabetic diet
Orders =
• O
2
therapy per nasal
cannula STAT
• 12-lead EKG
• Serial troponin levels
• Sputum for gram stain, now
• Complete Blood Count
(CBC)
• Finger-stick glucose
• Chest X-ray
• Continuous telemetry
monitoring
• Long-acting insulin
• Regular insulin on sliding-
scale
• Atorvastatin
Enter the provided orders for this patient into his
record

26
Critical Task
Scenario Information
Usability Test Task
• Vitamins
• Aspirin
• Azithromycin
• 1800-calorie diabetic diet
Scenario 1, Part I: Emergency Department Nurse
Participant is now logged in as the ED Nurse
Critical Task
Scenario Information
Usability Test Task
ED nurse documents
medication administration,
O
2
therapy, EKG
performed, lab specimens
obtained, glucose test
performed, and telemetry
monitoring
Treatments & tests
performed =
• Continuous O
2
therapy
per nasal cannula initiated
• Continuous telemetry
monitoring initiated
• 12-lead EKG completed
• Finger-stick glucose
completed
Lab specimens collected =
• Serial troponin level
• Sputum for gram stain
• Complete Blood Count
(CBC)
Medications administered =
• Regular insulin on
sliding-scale
• Atorvastatin
• Vitamins
• Aspirin
•
Azithromycin
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided information for medication
administration, O
2
therapy initiated, EKG
completed, finger-stick glucose completed (and
result), and specimens collected for this patient
into his record

27
Scenario 1, Part I: Emergency Physician
Participant is now logged in as the ED Physician
Critical Task
Scenario Information
Usability Test Task
ED physician reviews
results of diagnostic tests
Diagnostic Test Results =
• Chest X-ray confirms
pneumonia
• Troponin is negative
• EKG shows abnormal,
but non-significant, ST
segment changes
• Sign on to the System
• Open the record for Mr. William John
• Find and review the provided diagnostic test
results
ED physician orders the
patient to be admitted as an
inpatient
Admit patient to Medical-
Surgical unit today for
observation and treatment
Enter admission order into the patient’s record
Scenario 1, Part II: Inpatient Nurse
Participant is now logged in as the Inpatient Nurse
Critical Task
Scenario Information
Usability Test Task
Inpatient nurse receives
the patient on the
Medical-Surgical unit and
verifies information
documented by the Triage
nurse, ED nurse, and ED
physician, and reviews
diagnostic test results and
the order for inpatient
admit
Patient = Mr. William John
Age = 65 years
Ethnicity = Hispanic
Sex = Male
• Sign on to the System
• Open the record for Mr. William John
• Find and verify the documented demographic
information
• Find and verify the documented patient
complaints, current illnesses/conditions,
allergy, vital sign, and O
2
saturation
information
• Find and review the documented medication
administration information
• Find and review the information documented
for the treatments and tests performed
• Find and review the diagnostic test results
• Find and verify the inpatient admit orders
Patient complaints = severe
chest pain, difficulty
breathing, and productive
cough
Current illnesses/conditions
(history) = Type 2 diabetes
mellitus,
hypercholesterolemia
Allergies = thimerosal and
“pink sweetener”
Temperature, Blood Pressure,
Respiratory Rate = within
normal limits for an adult
male
28
Critical Task
Scenario Information
Usability Test Task
Heart rate = 110 BPM
O
2
Saturation = 90%
Treatments & tests performed
=
• Continuous O
2
therapy per
nasal cannula initiated
• Continuous telemetry
monitoring initiated
• 12-lead EKG completed
• Finger-stick glucose
completed
Medications administered =
• Regular insulin on sliding-
scale
• Atorvastatin
• Vitamins
• Aspirin
• Azithromycin
Diagnostic Test Results =
• Chest X-ray confirms
pneumonia
• Troponin is negative
• EKG shows abnormal, but
non-significant, ST
segment changes
Admission order = Admit
patient to Medical-Surgical
unit today for observation and
treatment
Inpatient nurse documents
vital signs information
and O
2
Saturation
information
O
2
Saturation = 98%
Enter the provided clinical information for this
patient into his record
Temperature, Heart Rate,
Blood Pressure, Respiratory
Rate information = within
normal limits for an adult
male

29
Scenario 1, Part II: Attending Physician
Participant is now logged in as the Attending Physician
Critical Task
Scenario Information
Usability Test Task
Attending physician makes
rounds and orders the O
2
Therapy changed to as
needed
Order = change O
2
therapy
per nasal cannula from
“continuous” to “prn, to
maintain O
2
Saturation >
96%”
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided O
2
therapy change order into
this patient’s record
Scenario 1, Part III: Inpatient Nurse
Participant is now logged in as the Inpatient Nurse
Critical Task
Scenario Information
Usability Test Task
On Day 2, the inpatient
nurse assesses the patient at
the beginning of the shift,
and observes that his right
eye is markedly pink, itchy,
irritated, and tearing; the
nurse documents these
findings
Suspecting viral
conjunctivitis, the nurse
puts the patient in contact
isolation and documents this
action
The nurse reports the
findings to the attending
physician and asks if she
wants an Ophthalmology
consult; based on the
physician’s verbal order, the
nurse orders the consult
Patient’s right eye is
markedly pink, itchy,
irritated, and tearing
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided information about the
patient’s eye into his record
• Enter the provided information about the patient
being placed on contact isolation into his record
• Enter into the patient’s record the provided
information about the condition of the patient’s
eye being reported to the physician
• Enter into the patient’s record the provided
information for verbal order on behalf of the
attending physician for an Ophthalmology
consult
Patient has been placed on
contact isolation
Condition of patient’s eye
reported to attending
physician
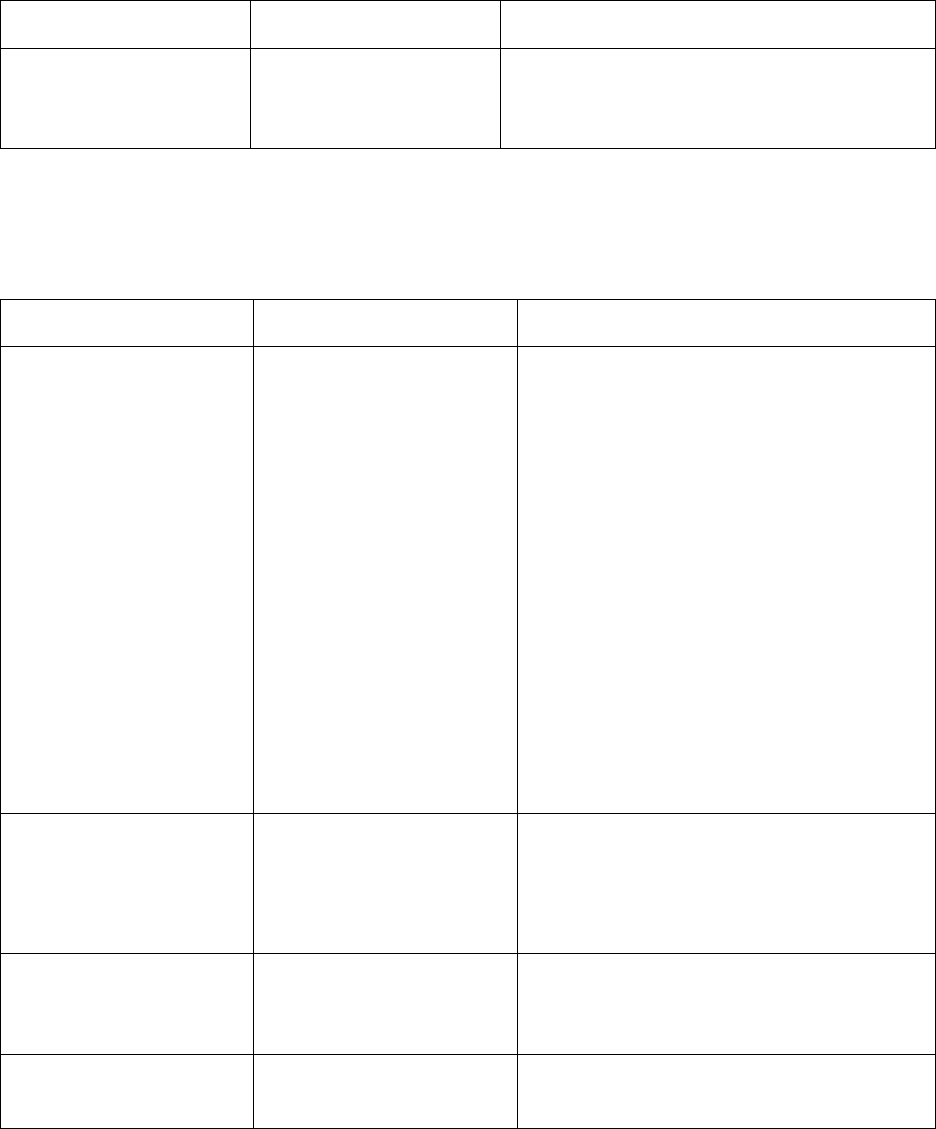
30
Critical Task
Scenario Information
Usability Test Task
Ophthalmology consult for
possible viral conjunctivitis
ASAP
Scenario 1, Part III: Ophthalmologist
Participant is now logged in as the Ophthalmologist
Critical Task
Scenario Information
Usability Test Task
The ophthalmologist
performs a consult and
documents her findings and
plan
• Patient has a history of
being in contact with a
family member who
recently had “pink eye”
• Patient was an occasional
contact lens wearer, but
has not been wearing
them recently
• Visual acuity, intraocular
pressure, and ophthalmic
exam are normal except
for signs and symptoms
consistent with viral
conjunctivitis
• Plan: will return
tomorrow or ask patient to
schedule a follow-up visit
in 24 hours if patient is
discharged before rounds
tomorrow
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided findings and Plan into this
patient’s record
The ophthalmologist orders
an eye medication
• Topical tetracaine 1%, to
be administered in both
eyes by ophthalmologist
(have bottles available in
patient’s medication tray
for physician’s rounds
Enter the provided order for the eye medication
into the patient’s record
The ophthalmologist orders
eye drops for the patient to
administer to himself
• Preservative-free artificial
tears in single-use vials
for patient self-
administration
Enter the provided order for the artificial tears
into the patient’s record
The ophthalmologist orders
an assay for adenovirus
• Keep an assay for
adenovirus available on
the patient’s hospital unit
Enter the provided order for the adenovirus assay
into the patient’s record

31
Scenario 1, Part IV: Attending Physician
Participant is now logged in as the Attending Physician
Critical Task
Scenario Information
Usability Test Task
Attending physician reviews
diagnostic test results, vital
signs, clinical observations
• Troponin levels
remained negative
• No change in the EKG
• Decreased chest pain and
cough
• Vital signs are normal
• Patient is stable
• Sputum culture and
susceptibility report is
positive for growth of
streptococcus
pneumoniae with
sensitivity to
azithromycin
• Blood cultures were
negative/no growth
• Sign on to the System
• Open the record for Mr. William John
• Find and review the provided clinical
information that is documented in the patient
record, including diagnostic test results, vital
signs, and other assessments
Attending physician
documents a discharge
summary
The troponin levels have
remained negative, and there
has been no change in the
EKG. Mr. John has
decreased chest pain and
cough, and other vital signs
are normal. The patient has
stabilized over the past 48
hours. The lab report for
sputum specimen is positive
for growth of streptococcus
pneumonia, with
confirmation of sensitivity to
azithromycin. The blood
cultures returned negative
with no growth. Patient to be
discharged home with a
diagnosis of pneumonia and
conjunctivitis.
Enter the provided discharge summary
information into the patient’s record
Attending physician orders
the patient to be discharged
from the hospital to home
with a final diagnosis of
pneumonia and
conjunctivitis, and with
instructions to schedule a
visit with his primary care
physician and a
Discharge patient to home
Final diagnosis pneumonia
and conjunctivitis
Patient to schedule a visit
with his primary care
physician in seven days
Enter the provided discharge order information
into the patient’s record

32
Critical Task
Scenario Information
Usability Test Task
recommendation to schedule
a visit with the
ophthalmologist the next
day for follow up on his
viral conjunctivitis
Recommended that patient
schedule a visit with the
ophthalmologist for
tomorrow for follow up on
the viral conjunctivitis

33
Use Case 2: Outpatient Care Testing (inpatient data is only to prepopulate hospital chart not
to test)
Scenario 2, Part I: Triage Nurse
Participant is now logged in as the Triage Nurse,
Critical Task
Scenario Information
Usability Test Task
Patient chart has been
“initiated”
Nurse documents patient’s
demographics
Patient = Mr. William John
Age = 67 years
Ethnicity = Hispanic
Sex = Male
• Sign on to the System
• Open the patient record for Mr. William John
• Enter/verify the provided demographic
information for this patient into the System
Nurse enters patient’s
complaints, current
illnesses/conditions (history),
and allergies
Patient complaints =
headache and reported two
short periods of confusion
Enter the provided clinical information for this
patient into his patient record
Current illnesses/conditions
(history) = Type 2 diabetes
mellitus,
hypercholesterolemia
Nurse documents triage
information with disposition
to Emergency Department
(ED)
Patient is triaged and taken to
the ED
Enter information into the patient’s record about
triaging and transporting him to the ED
Scenario 2, Part I: Emergency Department Nurse
Participant is now logged in as the ED Nurse
Critical Task
Scenario Information
Usability Test Task
ED nurse records the
patient’s vital signs
Temperature, Heart Rate,
Blood Pressure, Respiratory
Rate = within normal limits
for an adult male
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided clinical information for this
patient into his record

34
Scenario 2, Part I: Emergency Physician
Participant is now logged in as the ED Physician
Critical Task
Scenario Information
Usability Test Task
ED physician orders lab
tests, a radiology test,
EKG, and other diagnostics
tests
Orders =
• Electrolytes
• Complete Blood Count
(CBC)
• Chest X-ray
• CT Scan of head
• EKG
• ECHO cardiogram
• Carotid artery Doppler
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided orders for this patient into
his record
Scenario 2, Part I: Internist
Participant is now logged in as the Internist
Critical Task
Scenario Information
Usability Test Task
Internist orders admit to
ICU and additional
diagnostics testing
Orders =
• Admit to ICU for
evaluation of possible
stroke or TIA
• MRI
• Sign on to the System
• Open the record for Mr. William John
• Enter the provided orders for this patient into
his record
Internist reviews results of
diagnostic testing
• Electrolytes results = low
Na
+
and K
+
• Complete Blood Count
(CBC) result = normal
• Chest X-ray = negative
• CT Scan of head =
negative
• EKG = negative
• ECHO cardiogram =
misfiled in media section
of patient record
• Carotid artery Doppler =
negative
Review the provided results in the patient record
Internist orders outpatient
diagnostic testing,
medication with teaching,
and discharge with follow-
up
Orders =
• MRI outpatient
• Coumadin with teaching
by pharmacist
• Discharge to home, final
diagnosis possible TIA
• Patient to schedule a visit
with his primary care
physician in seven days
Enter the provided discharge orders for this patient
into his record

35
Critical Task
Scenario Information
Usability Test Task
• Patient to schedule a visit
with neurologist in three
days
Scenario 2, Part II: Primary Care Physician
Participant is now logged in as the Primary Care Physician
Critical Task
Scenario Information
Usability Test Task
Primary care physician
looks for diagnostic results
from tests performed in the
hospital
• MRI and ECHO
cardiogram results not
available
• Electrolytes results = low
Na
+
and K
+
• Complete Blood Count
(CBC) result = normal
• Chest X-ray = negative
• CT Scan of head =
negative
• EKG = negative
• ECHO cardiogram =
misfiled in media section
of patient record
• Carotid artery Doppler =
negative
• Sign on to the System
• Open the record for Mr. William John
• Search for MRI and ECHO cardiogram results
in the patient’s record
• Review the provided results that are available in
the patient’s record
Primary care physician is
interrupted by call from
Emergency department
regarding Mr. Bates who
has presented with a nose
bleed.
Physician moves to Mr.
Bates chart. Physician opens
Mr. Bates chart and reviews
his history and medication.
• Physician opens Mr. Bates chart for review
• Physician closes Mr. Bates chart and is able to
go back to Mr. William Johns chart.

36
6 Empirically Based Human Factors Guidance for Safety-
Enhanced Design of Health Information Technology
Human factors guidance for safe and usable design exists for a number of safety-critical
domains, but not currently for health information technology (HIT) design. For example,
the Human Factors Design Standard (HFDS) is a compilation of human factors principles
and guidance for the procurement, design, development, and testing of aviation systems,
facilities, and equipment.
22
Within this document, the principle of ‘simplicity’ is defined
as “Information should be presented simply and in a well-organized manner.” In order to
achieve this principle, the following guidance is provided, along with other
recommendations: "Information should be presented in consistent, predictable locations.”
Based upon our empirical findings, detailed in the previous section, as well as a
comprehensive review of existing standards under NIST Contract Number
SB134110CN0107, we provide a limited set of high-priority guidance below. These
guidelines for standardization are targeted uniquely at eliminating ‘never events’ and
associated patient harm by proactively addressing and mitigating the root causes of
critical use errors from EHR design and implementation elements, as distinguished in our
framework on the relationship between usability and patient safety, as described in Figure
3 of NISTIR 7804 Technical Evaluation, Testing and Validation of the Usability of
Electronic Health Records.
23
The empirically based human factors guidance for safety-enhanced design is:
1. Consistently display information critical to patient identification in a reserved area (specified
below) to avoid wrong patient errors
1.1 Patient identification information shall be displayed in the upper left hand corner of
all screens/windows in a consistent order; so that users can efficiently and accurately
find and verify patient identity
1.2 The information shall continue to be displayed in the same location regardless of
scrolling or other navigational mechanisms to move within the screen/window
1.3 The order shall be to first display the patient’s name with the last (family) name
capitalized, followed by a comma and then first (given) name, middle name, and
modifier, followed by date of birth using e.g., Nov 9, 1961 format and age and
gender, and then followed by MRN number.
1.4 For mobile devices or tablets with smaller screen sizes, it may be preferable to display
the information horizontally using the same ordering convention and white space
between the three elements. The information should be demarcated on the bottom
37
and/or the side, such as by employing white space, shading, or a line, from additional
optional identifiers
1.5 An example of this reserved area is:
SMITH, Walter Joseph III
Nov 9, 1961 (53 yo M)
MRN1348887
a. NAME: The last (family) name should be first and capitalized followed by a ‘,’ and
space prior to a capitalized first (given) name with the rest of the name in lower
case. The capitalization is used to distinguish the last name in cases of ambiguity
(e.g., Clark Kelly could be Clark KELLY or Kelly CLARK). It also reduces variation for
names with multiple capitalizations, such as McDonald.
b. NAME MODIFIER: In the absence of a modifier (e.g., Jr, Sr, III), nothing shall be
displayed in that location
c. DATE: The month represented as the first three letters of the month (or four in
languages other than English such as Italian where this is needed to
disambiguate months) shall be represented with a capitalized first letter with the
rest in lower case in order to make the capitalized last name more distinguishable
quickly on the display. The full year shall be displayed as four numeric digits
d. AGE: Displaying the age reduces the cognitive work required by the user to
convert date of birth into age. For years old, the display convention is ‘yo’ with a
space after the number, rounded down to the nearest digit. Similarly, months old
is displayed as ‘mo’, weeks old as ‘wo’, and days old as ‘do’. In Neonatal Intensive
Care Units, DOL 1 is often used for the first day of life, which corresponds to 0
days old. Similarly, DOL 2 is the second day of life. Decisions on when to display
yo, mo, wo, do, and DOL are expected to vary by institution. For example, a
hospital may display DOL for the first five days of life, followed by do until 30
days old, then wo until 24 weeks old, then mo until 24 months old, and finally yo
after 24 months of age. For the purposes of tracking accuracy of information, it
should be possible to display ‘on demand’ the value of the age in the original
format in which it was stored or transferred with interoperable systems. Age for
patients should not be displayed in values of less than 1 unit (e.g., 0.0001 yo)
e. GENDER: For gender, the display options should be M or Male for Male, F or
Female for Female, and Other. Additional details specifying subcategories under
Other, as necessary, shall be viewable on demand, such as transgender, or
reasons for a gender change
f. MRN: The allocation of digits to the Medical Record Number (MRN) should be
able to be modified in the future to accommodate future changes. Additional
identifiers such as care episode can be included on this line after the MRN. The

38
font size for MRN and other numeric identifiers can be smaller than the other
information displayed in the reserved area or placed to the right of the name and
date of birth information, but should still be viewable by older users.
4
MRN
information may be displayed in the reserved area only in response to an explicit
user action and/or when a barcoded wristband is scanned. Other identifiers, such
as encounter numbers, shall not be displayed in the reserved area in order to
reduce the likelihood of confusing the identifiers
g. ADDITIONAL IDENTIFIERS: Optional additional identifiers shall not be included in
the reserved area, as defined by being below a clearly demarcated horizontal line
or to the right of the area above the demarcation line. The display of optional
identifiers should not cover task-critical information except for short periods ‘on
demand.’ Additional optional identifiers include:
1) Place of birth
2) Picture. Note: Recommended to be a color picture of an individual patient
taken within the last 5 years, with no other individuals in the picture, and as a
close-up of the head facing the camera.
3) Biometrics
4) Genome
5) Barcode
6) Episode/encounter code
7) Suspected, confirmed or ruled out to have a highly infectious disease (e.g.,
‘Confirmed Ebola’), etc.
4
Kochurova, Olga, Joan K. Portello, and Mark Rosenfield. "Is the 3× reading rule appropriate
for computer users?." Displays 38 (2015): 38-43.

39
2. Provide visual cues to reduce risks of entering information and writing orders in the wrong
patient’s chart
2.1 Visually differentiate a chart
5
that enables a user to have unrestricted access to input
information (i.e., input mode) from a chart, which restricts the user’s ability to input
information (i.e., view-only mode)
2.2 Enable user to enter information on only one patient’s chart at one time
2.3 Enable user to have a chart in view-only mode in parallel with a chart with unrestricted
access to input information in order to support specialty-specific care needs (e.g.,
coordinated mother and child care following a birth, coordinated care of multiple birth
patients)
2.4 Enable user to easily transition from the current chart with unrestricted access to input
information to another chart by a deliberate action (i.e., identification/activation of the
patient chart), by the user.
2.4.1 Categories of charts that are likely to be needed by clinical providers are
1) charts for patients that are scheduled to be seen in the near future (e.g.,
24 hours), 2) charts for patients that have recently had information input
into them, 3) charts that have ordered laboratory tests or imaging tests
that are pending results, and 4) charts that have planned actions such as
documenting progress notes which have not yet been completed.
2.4.2 Easily transition implies that context has to be preserved in a way that is
clear to the user when the user transitions to another chart and back to a
previous chart; and that it is easy to find and identify a desired patient's
chart for any relevant patient in the system. Context should be preserved
in these transitions such that unsaved work in progress text should be
preserved by the system until saved (or deleted) by the user
2.5 Visually distinguish the mechanism for moving within a single patient’s chart and
transitioning from one chart with unrestricted access to input information to another
5
In the 2002 article "Maintaining a Legally Sound Health Record." Journal of AHIMA 73(2), a
chart is defined as "generated at or for a healthcare organization as its business record and is the
record that would be released upon request. It does not affect the discoverability of other
information held by the organization. The custodian of the legal health record is the health
information manager in collaboration with information technology personnel. HIM professionals
oversee the operational functions related to collecting, protecting, and archiving the legal health
record, while information technology staff manage the technical infrastructure of the electronic
health record."

40
3. Support efficient and easy identification of inaccurate, outdated, or inappropriate items in lists
of grouped information by having information presented simply and in a well-organized
manner.
Ways to achieve this include the following:
3.1 Lists of patients assigned to a particular clinician user should be presented in consistent,
predictable locations within and across displays and print-outs and the content should
not vary based on display location.
3.2 The status of a note and order as draft as compared to final shall be clearly indicated on
appropriate displays.
3.3 Clearly indicate the method by which the system saves information, whether auto-save or
requiring deliberate action to save, or combinations thereof.
3.4 Inputted information should be automatically saved when a user transitions from one
chart to another.
3.5 The language used should be task-oriented and familiar to users, including being
consistent with expectations based upon clinical training.
3.6 Enable a user to easily order medications that have a high likelihood of being the
appropriate medication, dose, and route. The likelihood is increased when displays are
tailored to specialty-specific user requirements, comply with national evidence-based
recommendations, are in accordance with system, organizational, unit, or individual
provider preferences specified in advance, or are similar to orders made by the same
physician on similar patients, on the same patient in the past, or providers with similar
characteristics.
3.7 Support assessing relationships of displayed information and allowing users with
appropriate permissions to modify locations and relationships for inaccurately placed
information, including laboratory results, imaging results, pathology results, consult
notes, and progress notes. This includes information within a single patient’s chart as well
as information placed in the wrong patient’s chart. The information about the time and
person that made the change should be viewable on demand.

41
7 Conclusions
This report examines the use of EHRs and their potential to improve and hinder healthcare
quality and patient safety. We drew upon five different methods of data collection, utilized
cross-cutting analytic methods, and had analysts from different disciplines and perspectives. The
results demonstrate strong congruence among the data, across the methods, and amongst the
analysts. Three major critical use risk areas surfaced during analysis: 1) Identification of
information; 2) Consistency of information; and 3) Integrity of information. These three areas
are consistent with findings from other studies that examined the use of EHRs.
Ultimately, the data from this study demonstrate that during safety-critical tasks and times,
patient safety is negatively affected, in part because mistakes and critical use errors occur more
frequently and because users are highly frustrated, and thus more likely to employ workarounds,
such as relying upon supplemental artifacts, e.g., paper ‘shadow charts’ or whiteboards. Figure 3
below highlights the ways in which problems with identification, consistency, and integrity of
information can result in suboptimal and unsafe patient care.
Figure 3. Relationship between usability findings and safe and effective clinical care
42
In accordance with the empirical evidence, and in order to make care more optimal and safe, we
provided human factors guidance for improving the usability of EHRs. There are three areas for
this guidance:
1) Consistently displaying information critical to patient identification in a reserved area to
avoid wrong patient errors,
2) Providing cues to reduce risks of entering information and writing orders in the wrong
patient’s chart, and
3) Supporting efficient and easy identification of inaccurate, outdated, or inappropriate
items in lists of grouped information by having information presented simply and in a
well-organized manner.
Finally, we provided two use cases for use during summative usability testing to achieve the goal
of safety-enhanced design by validating that potential patient safety risks are proactively
addressed and/or mitigated, one for the inpatient setting and one for the outpatient setting. These
use cases may also prove useful for organizations that tailor aspects of the design during
implementation and optimization processes to protect against inadvertently introducing new risks
to patients.

43
8 References
1
Buntin, M., Burke, M., Hoaglin, M., & Blumenthal, D. (2011). The benefits of health
information technology: a review of the recent literature shows predominantly positive results.
Health Affairs, 30 (3), 464-471.
2
Gibbons, M.C., et al. (2009). Impact of consumer health informatics applications. Evidence
Report/Technology Assessment, Oct (188), 1-546; and Cebul, R., Love, T., Jain, A.K., & Hebert,
C.J. (2011). Electronic health records and quality of diabetes care. New England Journal of
Medicine, 365, 825-833.
3
Longhurst, C., Parast, L., Sandborg, C., et al. (2010). Decrease in hospital-wide mortality rate
after implementation of a commercially sold computerized physician order entry system.
Pediatrics, 126, 14-21.
4
Institute of Medicine. (2001). Crossing the quality chasm: a new health system for the twenty-
first century. Washington, DC: National Academy Press.
5
Classen, D.C., et al. (2011). Global trigger tool shows that adverse events in hospitals may be
ten times greater than previously measured. Health Affairs, 3(4), 581-589.
6
Han, Y.Y., Carcillo, J., Venkataraman, S., et al. (2005). Unexpected increased mortality after
implementation of a commercially sold computerized physician order entry system. Pediatrics,
116(6), 1506 –1512. Correction in Pediatrics, 117(2), 594.
7
Horsky J, Kuperman GJ, Patel VL. Comprehensive analysis of a medication dosing error
related to CPOE. J Am Med Inform Assoc 2005; 12(4):377-82.
8
Hruschka, D. J., Schwartz, D., Cobb St. John, D., Picone-Decaro, E., Jenkins, R. A., Carey, J.
W. (2004). Reliability in coding open-ended data: Lessons learned from HIV behavioral
research. Field Methods, 16, 307-331.
9
Erlandson, D. A., Harris, E. L., Skipper, B. L., & Allen, S. D. (1993). Doing naturalistic
inquiry. Thousand Oaks, CA: Sage.
10
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Thousand Oaks, CA: Sage.
11
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative
analysis. Thousand Oaks, CA: Sage.
12
Saldaña, J. (2013). The coding manual for qualitative researchers. Thousand Oaks, CA:
Sage.
13
Saldaña, J. (2013). The coding manual for qualitative researchers. Thousand Oaks, CA:
Sage.
14
Richards, L., & Morse, J. M. (2007). User’s guide for qualitative methods (2
nd
ed). Thousand
Oaks, CA: Sage.
15
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative
analysis. Thousand Oaks, CA: Sage.
16
Saldaña, J. (2013). The coding manual for qualitative researchers. Thousand Oaks, CA:
Sage.
17
Saldaña, J. (2013). The coding manual for qualitative researchers. Thousand Oaks, CA:
Sage.
18
Saldaña, J. (2013). The coding manual for qualitative researchers. Thousand Oaks, CA:
Sage.
19
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Thousand Oaks, CA: Sage.
20
Patton, MQ. (1999). Enhancing the quality and credibility of qualitative analysis. HSR: Health
Services Research, 3, 1189-1208.

44
21
Mays, N. & Pope, C. (2000). Qualtative research in health care: Assessing quality in
qualitative research. BMJ: British Medical Journal, 320, 50-52.
22
Ahlstrom, V., & Longo, K. (2003). Human Factors Design Standard (HF-STD-001). Atlantic
City International Airport, NJ: Federal Aviation Administration William J. Hughes Technical
Center.
23
Svetlana, L.Z., Matthew, Q.T., Ramaiah, M., Schumacher, R.M., Patterson, E.S., North, R.,
Zhang, J., Gibbons, M.C., Abbott, P. “NISTIR 7804 Technical Evaluation, Testing and
Validation of the Usability of Electronic Health Records.” NIST Interagency/Internal Report
(NISTIR) 7804, 2012. Available at: http://www.nist.gov/customcf/get_pdf.cfm?pub_id=909701.
