
Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Department of Human Services
Division of the Deaf and Hard of Hearing
Equipment Distribution Program
Eligibility Application
The New Jersey Division of the Deaf and Hard of Hearing (DDHH) provides free assistive
devices to deaf or hard of hearing individuals through the Equipment Distribution Program
(EDP). Since 1993, the DDHH has operated this program to ensure that New Jersey residents
with hearing loss have access to critical telecommunications and vital home safety alerting
equipment. Upon meeting program eligibility, individuals receive communication devices at no
cost.
Program Eligibility:
Must have hearing loss
Must be a New Jersey resident
Total combined household income must not be greater than 400% of the federal poverty
level.
Please complete the application using the checklist below:
☐ A copy of ONE (1) document from List A to establish residency and identity. (Page 2)
☐ OR a copy of ONE (1) document from List B to establish identity AND a copy of ONE (1) document to
establish residency. (Page 2)
☐ Applicant’s signature (Page 2)
☐ Include email address for UPS tracking updates (Page 3)
☐ Certification of Disability completed by treating provider, with signature. (Page 4)
☐ Review of Conditions of Acceptance, with signature. (Page 5)
☐ Items selected (Pages 6-9)
☐ Joint or individual copy of most recent tax return or W2s showing household income or a letter from
your Employer or Award Letter from a Social Service Agency or US Department of Veterans Affairs.
☐ Submit application by mail, fax, or email:
DDHH Equipment Distribution Program
PO Box 074
Trenton, NJ 08625-0074
Fax: 609-588-2528
Email: DDHH.communications2@dhs.nj.gov
Number of people living in household
2024 Federal Poverty Guidelines
1
$60,240
2
$81,760
3
$103,280
4
$124,800
5
$146,320
*For each additional person, add $21,520
Source U.S. Department of Health and Human Services

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
SECTION 1: Please provide a copy of one (1) document from List A OR a copy of one (1) document
from List B AND a copy of one (1) document from List C.
List A
Documents that establish both
identity and residency
Please select one from the list
below
NJ or Municipal ID card
NJ Driver's License
NJ Student ID
Utility, cell phone, or
internet bill
Bank/insurance statement
Tax Returns, last two years
Paystub from employer
Rent receipt, lease,
mortgage
Letter from social service
agency
Letter from health care
provider
Letter from government
agency
List B
Documents that
establish identity
Please select one from the
list below
Student ID card
Student
Transcript
Passport
Birth Certificate
Driver License
from another
country
Consulate ID
card
A child's U.S.
birth certificate
and your name
Letter from IRS
or ITIN
Marriage
Certificate
Divorce Decree
U.S. court
document
List C
Documents that
establish residency
Please select one
from the list below
Signed and dated
letter including the
full name and
phone number of
the individual
writing the letter
from one of the
following:
•
Landlord
•
Representative
of worship
•
Medical
provider
•
Service
provider
•
Shelter
acknowledging NJ
residency

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program
Application Form
SECTION 2: This form will be scanned for computerized data capture. Please follow the instructions to
ensure that the application is processed quickly and accurately.
Use blue or black ink only.
Print clearly, in uppercase letters.
Correct errors with white correction fluid.
First Name: _______________________________ Middle Initial: _____
Last Name: _______________________________
Telephone Number: ________________________
Check one: ☐ Cell ☐ Home ☐ Videophone
Email Address: ____________________________
IMPORTANT: Email addresses will be used to provide UPS tracking updates.
How do you identify: ☐ Deaf ☐ Hard of Hearing
Check one: ☐ Mild ☐ Moderate ☐ Profound ☐ Unable to speak or sign
Mailing Address
Street: ___________________________________ City: _______________________
County: __________________________________ Zip Code: ______________
Physical Address (if different from Mailing Address)
Street: ___________________________________ City: _______________________
County: __________________________________ Zip Code: ______________
I certify to the best of my knowledge that I meet the program’s eligibility requirements and the
information in this application is true and correct.
Applicant’s Signature: Date:

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program Form
Certification of Disability
SECTION 3: This portion of the application must be completed by a treating service provider. Provider,
please verify and certify that the applicant will benefit from the use of the requested technology.
This form will be scanned for computerized data capture. Please follow the instructions to ensure that
the application is processed quickly and accurately.
Use blue or black ink only.
Print clearly, in uppercase letters.
Correct errors with white correction fluid
Applicant’s Name: ___________________________________
Provider’s Information:
First Name: _______________________________ Middle Initial: _____
Last Name: _______________________________
Business Information:
Street: ___________________________________ City: _______________________
County: __________________________________ Zip Code: ______________
Telephone Number: ________________________ Fax Number: __________________
Email Address: ____________________________
Certification/License Number: ______________________________
Expiration Date (MM/DD/YY): ______________________________
Provider’s Profession:
☐ Doctor/Physician
☐ Audiologist
☐ Hearing Aid Specialist Speech
☐ Pathologist
☐ Other (please describe):
_____________________________
Signature _______________________________________ Date: ___________________

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program
Conditions of Acceptance
SECTION 4: Please review the following section in its entirety.
I understand and agree to the following:
Equipment is the property of the State of New Jersey. I will not sell, pawn, give, or loan the
equipment to individuals outside of my household. If I do, I understand I can be criminally
prosecuted.
The NJ DDHH is not responsible for service plans or bills associated with equipment.
I will protect the equipment from damage.
If the equipment is not working, I will NOT try to repair it or take it apart. I will contact DDHH for
instructions on returning the equipment. Equipment, including all accessories, should be returned
to the manufacturer in its original box if the warranty has not expired.
If the equipment is returned and NJ DDHH determines it has been damaged, a replacement will
NOT be allowed.
If the equipment is reported as lost, a replacement will NOT be allowed.
If the equipment is stolen or damaged by someone other than me, I will report it to the police and
provide a copy of the police report to NJ DDHH before replacement is allowed.
It is against the law to file false statements. If I provide false statements in this application or
regarding equipment, I understand I can be criminally prosecuted.
I agree to indemnify the State of New Jersey from any and all claims, damages, and expenses
that arise out of the use or misuse of equipment by myself or anyone else.
If there is a change in address or phone number, I will provide the new information to NJ DDHH
within 30 days.
If I move to another state, I will contact NJ DDHH to arrange the return of equipment before I
move.
If I am a minor, all equipment, obligations, and responsibilities will be transferred to me when I
turn 18.
I will make arrangements to return my equipment in the event of my death.
Households must wait five (5) years before receiving another phone through this program.
A limit of one (1) smoke detector or baby alert system is provided within this program.
If I fail to follow these Conditions of Acceptance, I can be denied the benefit of having equipment
offered by the NJ DDHH.
Applicant’s Signature: _______________________________ Date: __________________

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program
Items Available Through EDP
The Sonic Alert HomeAware Fire and CO Signaler is a
flashing strobe light with a built-in smoke / CO listener,
phone, and bed shaker. This device is for use with
existing smoke detector and/or CO2 alarm system.
The Nighthawk 900-0230 is a battery-operated carbon
monoxide alarm that provides reliable protection
against the dangers of carbon monoxide, and has a 7-
year limited warranty. It is recommended that this item
be paired with the Sonic Alert HomeAware device.
The Ring Video Doorbell 2 is a smart security system
that can be monitored from anywhere. The doorbell is
battery powered with the option to hardwire and comes
with a rechargeable battery pack.
The Sonic Alert is perfect for smoke alerts in other
rooms. This does not replace existing smoke
detectors. This will pair well with the HomeAware alert
listener system.
Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program
Items Available Through EDP
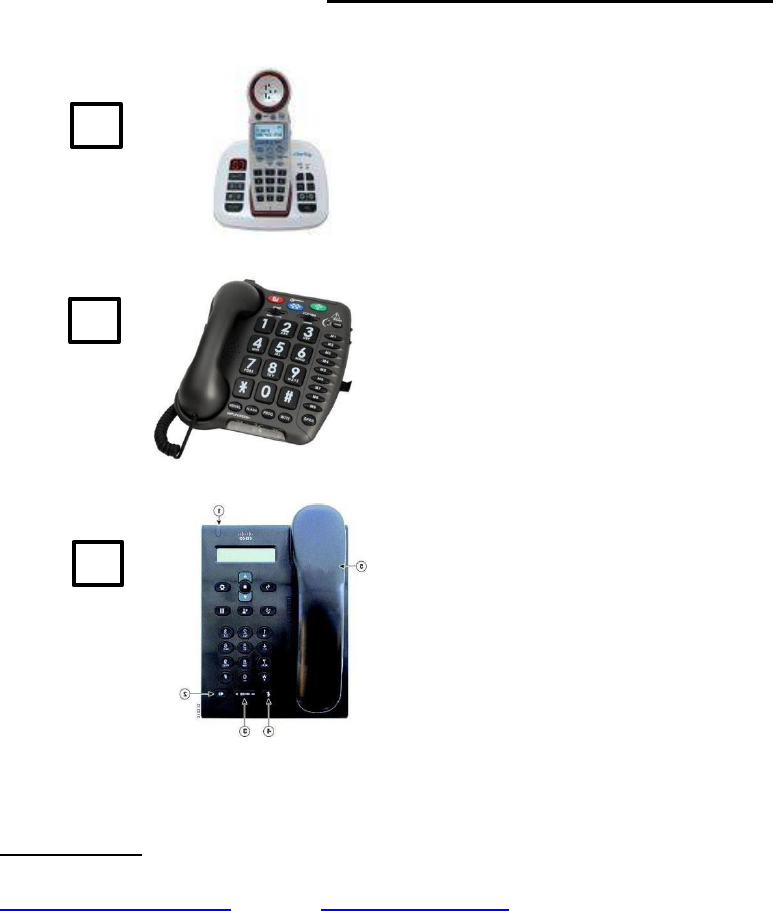
The Clarity XLCR Amplified Cordless Extra Loud
(50dB) phone with tone control including 4 settings,
boost button, and volume control wheel to give provide
a customized listening experience
The Geemarc Amplipower 60 Plus Amplified
Telephone has a receiver volume control of up to 67dB
and an adjustable ringer volume. The speaker offers
clearer reception and tone control of plus or minus 10
dB.
The Cisco Unified SIP Phone 3905 provides
accessibility features for the hard of hearing, blind, and
mobility impaired. Because many of these features are
standard, they can be used by users with disabilities
without requiring special configuration.
IMPORTANT: Unfortunately, the CapTel 840+ is no longer in service. Please contact Customer Service
at CapTel for more information. Captel can be reached via phone at (888) 269-7477, email
contact CapTel to request an upgrade to an internet model.

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program
Items Available Through EDP
The Minicom IV has an easy-touch keyboard with a
bright, tilted 20-character display and includes a printer
port to connect an external printer.
VTech DM221 Digital Audio Baby Monitor is a simple,
2-piece baby monitoring system that works great for
deaf & hard of hearing parents or caregivers

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
New Jersey Equipment Distribution Program
Choose ONE from this list:
Tablet - Apple iPad Wi-Fi Only 64GB
* Requires Access to Internet Service.
Tablet - Samsung Galaxy S6 Lite Wi-Fi Only
64GB *Requires Access to Internet Service.
Smartphone - Apple iPhone XR Wi-Fi & 4G
64GB *Requires Cellular Service Plan.
Smartphone - Google Pixel 5a Wi-Fi & 4G
128G B *Requires Cellular Service Plan.
IMPORTANT:
If a Smartphone is selected, the individual must agree to get a cellular service plan from a provider. The
tablets are Wi-Fi only and do not require a service plan. All Smartphones offered in this program are
“unlocked” so that the individual may choose a service provider of their choice.
For individuals who need low-cost internet service there may be an option through the FCC
Emergency Broadband Benefit - https://www.fcc.gov/broadbandbenefit
The device will come with the following deaf and hard of hearing accessible apps pre-installed:

Division of the Deaf and Hard of Hearing
New Jersey Equipment Distribution Program
IP Relay, Video Relay Service, IP Captioned Telephone Service, Video Calls & Video
Messaging.
All devices include a 3-year warranty. DDHH does not provide cases. We urge you to
purchase a protective case for the device selected. These devices are subject to breakage if
they are dropped. DDHH will not replace a device that is damaged due to breakage.
SECTION 5: If you are assisting someone else in completing this application, please complete the
following portion.
This form will be scanned for computerized data capture. Please follow the instructions to ensure that
the application is processed quickly and accurately.
Use blue or black ink only.
Print clearly, in uppercase letters.
Correct errors with white correction fluid
1. Please check one of the following boxes regarding relationship to the applicant.
☐ Family Member
☐ Friend
☐ Attorney
☐ Agency
☐ Advocate
☐ Social Worker
☐ Other (please specify):
_________________
Last Name: _______________________________ Suffix (Jr., Sr., etc.): ________
First Name: ___________________________ Middle Initial: ____
Street Address: _______________________________________
City: ________________________________ State: ______ Zip Code: _________
Preparer’s Signature: _________________ Phone Number: ____________________
PLEASE SUBMIT THE FORM BY:
MAIL:
Division of the Deaf and Hard of Hearing
Equipment Distribution Program
PO Box 074
Trenton, NJ 08625-0074
EMAIL:
OR FAX:
(609) 588-2528
FOR MORE INFORMATION, CALL:
(609) 588-2648
(800) 792-8339
(609) 503-4862 videophone
