
doi: 10.1111/cea.12494 Clinical & Experimental Allergy, 45, 547–565
BSACI GUIDELINE
© 2015 John Wiley & Sons Ltd
BSACI guideline for the management of chronic urticaria and angioedema
R. J. Powell
1
, S. C. Leech
2
, S. Till
3
, P. A. J. Huber
4
, S. M. Nasser
5
and A. T. Clark
6
1
Department of Clinical Immunology and Allergy, Nottingham University, Nottingham, UK,
2
Department of Child Health, Kings College Hospital, London,
UK,
3
Division of Asthma, Allergy and Lung Biology, Kings College London, London, UK,
4
BSACI, British Society for Allergy & Clinical Immunology, London,
UK,
5
Department of Allergy & Clinical Immunology, Addenbrooke’s NHS Trust, Cambridge, UK and
6
Department of Allergy, Addenbrookes NHS Trust,
Cambridge, UK
Clinical
&
Experimental
Allergy
Correspondence:
Dr A. T. Clark, Allergy Clinic,
Cambridge University Hospitals NHS
Foundation Trust, Box 40, Cambridge
CB2 2QQ, UK.
E-mail: [email protected]
Cite this as: R. J. Powell, S. C. Leech,
S. Till, P. A. J. Huber, S. M. Nasser and
A. T. Clark, Clinical & Experimental
Allergy, 2015 (45) 547–565.
Summary
This guidance for the management of patients with chronic urticaria and angioedema has
been prepared by the Standards of Care Committee of the British Society for Allergy and
Clinical Immunology (BSACI). The guideline is based on evidence as well as on expert
opinion and is aimed at both adult physicians and paediatricians practising in allergy.
The recommendations are evidence graded. During the development of these guidelines,
all BSACI members were included in the consultation process using a Web-based system.
Their comments and suggestions were carefully considered by the Standards of Care
Committee. Where evidence was lacking, a consensus was reached by the experts on the
committee. Included in this management guideline are clinical classification, aetiology,
diagnosis, investigations, treatment guidance with special sections on children with urti-
caria and the use of antihistamines in women who are pregnant or breastfeeding. Finally,
we have made recommendations for potential areas of future research.
Keywords adult, allergy, angioedema, antihistamine, anti-IgE, auto-antibody, autoimmune,
breastfeeding, BSACI, child, epidemiology, guideline, hypothyroidism, IgE, management,
paraprotein, pregnancy, pregnancy, Urticaria
Submitted 6 October 2014; revised 11 December 2014; accepted 9 January 2015
Introduction
This guidance for the management of patients with
chronic urticaria/angioedema is intended for use by
physicians treating allergic conditions. It should be rec-
ognized that patients referred to an allergy clinic often
have a different pattern of presentation (e.g. intermit-
tent acute) from those referred elsewhere and both the
patient and referring practitioners often wish to deter-
mine whether allergy is involved.
Evidence for the recommendations was collected by
electronic literature searches of MEDLINE and EMBASE
using these primary key words: urticaria, angioedema,
angioneurotic oedema, allergy, allergic, antihistamines,
auto-antibody, autoimmune, hypothyroidism, IgE,
paraprotein, pregnancy, breastfeeding, child, epidemiol-
ogy, management, psychology. In addition, hand
searches were performed and the Cochrane library and
NHS evidence were also searched. Each article was
reviewed for suitability by the first and second author
of this guideline. The recommendations were evidence
graded at the time of preparation of these guidelines
(Appendix Tables B1 and B2). During the development
of these guidelines, all BSACI members were consulted
using a Web-based system and their comments and
suggestions were carefully considered by the Standards
of Care Committee (SOCC). Where evidence was
lacking, a consensus was reached among the experts
on the committee. Conflict of interests were recorded
by the SOCC. None jeopardized unbiased guideline
development.
Executive summary and recommendations
(Grades of recommendations are described in Appendix
Tables B1 and B2)
•
Chronic urticaria/angioedema has traditionally been
defined as weals, angioedema or both with daily or
almost daily symptoms lasting for m ore than 6 weeks.
In these guidelines, we have also included patients with
episodic acute intermittent urticaria/angioedema lasting
for hours or days and recurring over months or years.
•
Weals and angioedema commonly occur together,
but may also occur separately.

•
Chronic urticaria affects 2–3% of individuals (lifetime
prevalence) and significantly reduces quality of life (QoL).
•
There are important differences in aetiology and
management in children compared to adults.
•
The diagnosis is based primarily on the clinical his-
tory. Investigations are determined by the clinical his-
tory and presentation, but may not be necessary.
•
Management must include the identification and/or
exclusion of possible triggers, patient education and a
personalized management plan (grade of recommenda-
tion = D).
•
Food allergy can usually be excluded as a cause of urti-
caria/angioedema if there is no temporal relationship to a
particular food trigger, by either ingestion or contact. Food
additives rarely cause chronic urticaria and angioedema.
•
Certain drugs can cause or aggravate chronic urti-
caria and/or angioedema, and hence, a detailed drug
history is mandatory.
•
Autoimmune urticaria/angioedema in older children
and adults is reported to account for up to 50% of
chronic urticaria and may be associated with other
autoimmune conditions such as thyroiditis.
•
Autoimmune and some inducible weals can be more
resistant to treatment and follow a protracted course.
•
The commonest type of angioedema without weals is
histaminergic.
•
Angioedema without weals is a cardinal feature of
hereditary angioedema (HAE) and typically involves
subcutaneous sites, gut and larynx. In Types I and II
HAE, levels of C4 and C1 inhibitor (functional and/or
antigenic) are low.
•
Angiotensin converting enzyme (ACE) inhibitors can
cause angioedema without weals resulting in airway
compromise. They should be withdrawn in subjects with
a history of angioedema (grade of recommendation = C).
ACE inhibitors are contraindicated in individuals with a
history of angioedema with or without weals.
•
Pharmacological treatment should be started with a
standard dose of a non-sedating H1-antihistamine
(grade of recommendation = A).
•
The treatment regime should be modified according
to treatment response and development of side-effects.
•
Higher than normal doses of antihistamines may be
required to control severe urticaria/angioedema (grade of
recommendation = B). Updosing with a single antihista-
mine is preferable to mixing different antihistamines.
•
If an antihistamine is required in pregnancy, the
lowest dose of chlorphenamine, cetirizine or loratadine
should be used (grade of recommendation = C).
•
If an antihistamine is required during breastfeeding,
it is recommended that either cetirizine or loratadine
are taken at the lowest dose. Whenever possible, chlor-
phenamine should be avoided during breastfeeding
(grade of recommendation = C).
Definition
Chronic urticaria/angioedema (CU) has traditionally
been defined as weals, angioedema or both lasting for
more than 6 weeks [1, 2]. Acute urticaria is an episode
of spontaneous weals lasting for <6 weeks and is not
considered further in this guideline. However, we have
included patients with episodic urticaria/angioedema
lasting for hours or days and recurring over months or
years. Although rarely life-threatening, chronic urti-
caria/angioedema lead s to both misery and embarrass-
ment and has a significant impact on an individual’s
quality of life [3–5]. Regrettably, this troublesome con-
dition is often trivialized. Box 1 lists the terminology
pertaining to urticaria referred to in this guideline.
Urticaria (‘hives’ or ‘nettle rash’) is characterized by a
red (initially with a pale centre), raised, itchy rash
resulting from vasodilatation, increased blood flow and
increased vascular permeability. Weals can vary in size
from a few millimetres to hand-sized lesions which
may be single or numerous. The major feature of urti-
caria is mast cell activation that results in the release of
histamine (and other inflammatory mediators); that in
turn accounts for the raised, superficial, erythematous
weals and accompanying intense pruritus. Angioedema
(tissue swelling) is the result of a local increase in vas-
cular permeability, often notable in the face, orophar-
ynx, genitalia and less frequently in the gastrointestinal
tract. These swellings can be painful rather than itchy.
Weals affect the superficial skin layers (papillary der-
mis), whereas angioedema can involve the submucosa,
the deeper reticular dermis and subcutaneous tissues.
Weals and angioedema often coexist, but either can
occur separately. Characteristically the weals arise
spontaneously and each lesion re solves within 24 h.
This contrasts with angioedematous swellings that can
persist for a few days.
When functional antibodies are demonstrated, this
suggests an autoimmune basis. In the commonest form
Box 1. Terminology dependent on how study popula-
tion was characterized
Term Abbreviation Definition
Chronic urticaria CU Encompasses CsU and CaU
Chronic spontaneous
urticaria (previously
called CiU – chronic
idiopathic urticaria)
CsU Not associated with
auto-antibodies
Chronic autoimmune
urticaria
CaU Associated with antibodies
to IgE/IgE receptor
Hereditary Angioedema HAE Typically associated with
C1 inhibitor deficiency
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
548 R. J. Powell et al

of the disease (chronic spontaneous urticaria – CsU),
there appears to be persistent activation of mast cells in
the skin, but the precise mechanism of mast cell trig-
gering in CsU is unknown. Functional auto-antibodies
against the high-affinity IgE receptor (FceR1) have been
demonstrated in 30–40% of patients with CU suggesting
an autoimmune basis (CaU) [6–8].
Urticaria and angioedema in adults
Prevalence
The lifetime prevalence for all types of urticaria is
8.8%, but CU only develops in 30–45% of these indi-
viduals [8–10].
Clinical classification
Urticaria may occur alone in about 50% of cases,
urticaria with angioedema in 40%, and angioedema
without weals in 10% [11, 12]. However, a study by
Sabroe et al. [13] found a much higher percentage
(85%) of patients with urticaria and angioedema.
Table 1 lists the clinical classification of chronic urti-
caria/angioedema.
Aetiology
Optimal management of chronic and acute intermittent
urticaria depends on a thorough understanding of clini-
cal presentation, aetiology, triggers and aggravating fac-
tors. Patients with chronic urticaria are often referred to
allergy clinics as cases of possible food allergy – ‘to find
out what they are allergic to’. Rarely is food allergy the
cause of chronic urticaria and can typically be excluded
on the basis of clinical history. Common triggers/aggra-
vating factors/associations for exacerbations of chronic
urticaria are intercurrent viral infections [14] and psy-
chological factors [15]. The aetiological classification of
chronic urticaria/angioedema is given in Table 2.
Mechanisms
The central effector cell is the dermal/submucosal mast
cell, which on degranulation releases preformed vasoac-
tive mediators such as histamine, a major mediator of
urticaria and angioedema. Subseq uently cytokines,
chemokines and membrane-derived mediators (leukotri-
enes and prostaglandins) are released, contributing to
both the early- and late-phase responses with extrava-
sation of fluid into the superficial tissues.
Table 1. Clinical classification of chronic
urticaria/angioedema
Description Type Examples of triggers
Spontaneous urticaria Spontaneous Stress, infection, drugs (e.g. NSAIDs)
Autoimmune urticaria Autoimmune None known
Inducible urticaria Aquagenic Contact with hot or cold water
Cholinergic Exercise, emotion
Cold Swimming in cold water, cold wind
Delayed pressure Sitting, lying, tight clothing
Dermographism Minor trauma
Exercise Physical exertion
Heat Hot bath/shower
Solar Sunshine
Vibratory Use of vibrating tools
Angioedema
without weals
Spontaneous Stress, infection, drugs (e.g. NSAIDs)
C1 inhibitor deficiency Trauma, surgical procedures, stress,
infection
C1 inhibitor
deficiency related to
paraproteinaemia
Trauma, surgical procedures, stress,
infection
Drugs ACE inhibitors, oestrogens, antipsychotic
drugs, statins, NSAIDs
Vasculitis* Urticarial vasculitis Infection, e.g. with hepatitis B/C or
streptococcus; drugs, e.g. penicillins,
allopurinol, quinolones or
carbamazepine; autoimmune diseases;
paraproteinaemia; malignancy
Rare syndromes* Cryopyrin-associated
periodic syndrome (CAPS)
Cold
Schnitzler syndrome
*Vasculitis and rare syndromes are differential diagnoses of chronic urticaria and angioedema.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 549

Whereas the mast cell component of urticaria is easily
recognized (itching and wealing) and usually responds to
antihistamines, swelling in the deeper layers of the skin
is more difficult to quantify and additional mechanisms
are probably involved. Several inflammatory mediators
increase microvascular permeability leading to plasma
leakage and oedema formation. Animal experiments
have shown that certain mediators, for instance LTB4
and C5a, cause plasma leakage via neutrophil-dependent
pathways in a manner that does not require the neutro-
phil to trav erse the vascular endothelium, i.e. adhesion of
neutrophils to the vessel wall is sufficient to initiate
plasma leakage [16, 17]. Hence antihistamines are less
effective in contro lling the angioedema probably due to
their inability to affect consequent non-histamine-
related tissue oedema.
An examination of lesional skin biopsies from both
chronic spontaneous and autoimmune urticaria reveals
perivascular infiltrates of CD4+ lymphocytes, mono-
cytes and granulocytes (neutrophils, basophils and eo-
sinophils). This contrasts with biopsies from patients
with urticarial vasculitis (~1% ca ses of urticaria) in
which there is typically a small vessel vasculitis often
with deposition of immunoglobulin and complement
[11]. However, some patients with vasculitis exhibit
only subtle changes with endothelial cell swelling, red
cell extravasation and possibly leukocytoclasia.
Autoimmune urticaria (CaU). IgG antibodies to the
alpha subunit of the IgE receptor on mast cells or less
commonly IgG antibodies to IgE have been documented
in approximately one-third of individuals with chronic
urticaria [7, 18–20]. These antibodies are disease spe-
cific with some studies suggesting that this subgroup of
patients experiences a more intense and protracted dis-
ease course [13]. The mechanism has been reviewed in
the EACCI task force position paper [21].
However, sera from subjects wi th chronic urticaria are
also able to degranulate mast cells through mechanisms
independent of both IgE and IgG although the precise
nature of these histamine-releasing factors remains
unknown [22], but in vitro studies have suggested activa-
tion of the classical complement pathway [23, 24].
Vasculitis/immune complex-associated urticaria. Com-
plement activation can media te or augment histamine
Table 2. Aetiological classification of chronic urticaria/angioedema
Aetiology Mechanism Examples Investigations
Spontaneous
(40–50% cases)
Unknown Typically negative
Autoimmune IgG auto-antibody to mast cell
IgE receptor or to IgE bound
to mast cells
Associated with autoimmune thyroiditis ANA, thyroid auto-antibodies
Physical stimuli Direct mast cell mediator release Exercise, heat, cold, pressure, aquagenic,
solar, delayed pressure, vibration,
dermographism
Challenge testing with
appropriate stimuli, e.g. ice
cube, exercise. Cryoglobulins
Drug induced Reduced kinin metabolism; elevated
leukotriene levels
ACE inhibitors (angioedema alone)
NSAIDs
Response to avoidance (may
be delayed for weeks or months)
Infection Complement activation due to immune
complex formation
Parasites, EBV, hepatitis B and C,
viral exanthems
Serology directed by clinical
history
Allergic IgE-mediated allergic contact urticaria Latex, animals, grass, food Skin tests, specific IgE to
allergen
C1 inhibitor deficiency
Genetic (i) Enhanced kinin production HAE Types I and II C4, C1 inhibitor
Genetic (ii) Activation of complement, fibrinolysis
and coagulation systems
HAE Type III C4, C1 inhibitor, Factor
XII studies may be useful
Acquired Binding of C1 inhibitor by paraprotein Associated with paraproteinaemia C4, C1 inhibitor, Paraprotein
in both blood & urine
Non-IgE-mediated mast
cell degranulation
Non-receptor-mediated Opiates, Adrenocorticotropic
Hormones (ACTH)
Response to avoidance
Vasculitis Small vessel vasculitis, deposition of
immunoglobulin and complement
Urticarial vasculitis FBC, ESR, renal function,
urinalysis, LFT, ASOT,
hepatitis B and C serology,
immunoglobulin electrophoresis,
autoimmune screen including
ANA, ANCA, C3, skin biopsy
Food constituent (rare) Unknown Salicylates/benzoates Response to exclusion and
subsequent reintroduction
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
550 R. J. Powell et al

release from mast cells via the anaphylatoxin C5a. This
inflammatory pathway is triggered by the interaction
between antibody and antigen to form immune com-
plexes for example in hepatitis C [25–27], hepatitis B
[28], EBV and possibly parasitic infections.
Inducible urticarias. Patients can have an inducible ele-
ment to their urticaria with triggering by heat, cold,
pressure, vibration, water, ultraviolet light, etc. These
urticarias are induced reproducibly after a specific
physical stimulus is applied [29]. Weals usually appear
immediately and characte ristically fade within 1 h.
However, delayed pressure urticaria develops more
slowly after physical pressure and lasts several hours or
days. Inducible urticarias may require higher dose anti-
histamine therapy and delayed pressure urticaria may
remain refractory.
Possible food triggers. Symptoms of chro nic urticaria/
angioedema are typically non-allergic with most
patients having spontaneous or autoimmune urticaria/
angioedema. Nevertheless, patients or their parents fre-
quently analyse foods and food additives eaten over the
previous 24 h or longer in the search for a connection
with the symptoms.
A detailed history us ually enables an IgE-mediated
food allergy to be excluded as a cause of urticaria/an-
gioedema. Specifically in IgE-mediated food allergy,
symptoms typically occur reproducibly within 60 min
of exposure to the offending food rather than coming
on overnight or being present first thing in the morn-
ing. Furthermore, symptoms do not last several days.
Also urticaria and angioedema associated with IgE-
mediated food allergic reactions seldom occur in isola-
tion, i.e. additional symptoms are usually present such
as oropharyngeal itching and discomfort, wheezing,
vomiting or abdominal pain. Therefore, unless there is a
close temporal relationship to a particular food trigger,
by either ingestion or contact, an IgE-mediated food
allergy can be excluded.
Exceptions include allergic reactions to allergens,
such as omega-5 gliadin in wheat and lipid transfer
proteins in plant-derived foods, which may occasion-
ally present as intermittent spontaneous urticaria/exer-
cise-induced anaphylaxis. As exertion is frequently a
cofactor for reactions to these allergens, the temporal
relation to ingestion may not be immediately obvi-
ous.
Allergy to Crustacea may behave similarly, although
in practice these allergens are less ubiquitous and a
temporal relationship between ingestion and urticarial
episodes is usually apparent. Allergy to aGAL in red
meat may cause delayed reaction with urticaria,
although this is currently believed to be rare in the Uni-
ted Kingdom [30].
Stress. Urticaria and angioedema can lead to significant
stress and the converse is also recognized, namely that
psychological stress can trigger or aggra vate urticaria.
Although psychological stress in isolation is unlikely
to be the sole trigger, a high frequency of patients with
CsU report a stressful event preceding the onset of CsU
[31] and the possibility of a causal influence of emo-
tional distress, especially of stressful life events, on the
course of skin diseases has long been postu lated [32].
Patients with CsU experience high rates of anxiety,
depression and somatoform disorders such as fibrom-
yalgia, with half of subjects with CsU being affected by
at least one of these conditions [33, 34]. Psychiatric
comorbidity appears to significantly increase QoL
impairment [35]. Compared to allergy patients, individ-
uals with CsU had more severe comorbidity and higher
levels of life event stress and perceived stress. Further-
more, an association between post-traumatic stress and
chronic spontaneous urticaria has also been reported
[36]. Psychological therapies could be considered in
addition to medical management.
Other putative causes. An underlying extraneous cause
for chronic urticaria cannot be identified in many
patients, but infections may play a role in certain cases.
When present, chronic infections such as dental sepsis,
sinusitis, urinary tract infections and cutaneous fungal
infections should be treated. However, exhaustive inves-
tigations sear ching for underlying infections are not
indicated. Candida colonization does not cause chronic
urticaria [37]. There is limited evidence that if Helicobact-
er pylori colonization is present, eradication may result
in an improvement in CU; hence, routine screening of
Helicobacter pylori is not recommended [38, 39].
Mechanisms specifically related to angioedema
occurring without weals
Angioedema without weals. Individuals with angioe-
dema without associated weals should specifically have
their medication and family history reviewed to identify
those on angiotensin converting enzyme (AC E) inhibi-
tors and those patients with hereditary ang ioedema
(HAE). NSAIDs and antibiotics can also induce angioe-
dema [40, 41]. Acquired forms of C1 inhibitor defi-
ciency can result from serum paraproteins that have
auto-antibody activity against C1 inhibitor. Immune
complex formation by IgG with tumour surface anti-
gens may result in complement consumption. Invest iga-
tions typically show reduced levels of complement C4
and may reveal low levels of C1 inhibitor.
Angioedema with ACE inhibitors. The incidence of ACE
inhibitor-induced angioedema may be as high as 0.68%
[42] as most cases were initially thought to occur in the
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 551
first weeks of treatment, but it is now appreciated that
later onset angioedema, occurring after many years of
uneventful drug use, is quite common [42–44]. The
mechanism underlying the angioedema is likely to be
due to the reduced metabolism of bradykinin; this effect
may also aggravate angioedema associated with HAE.
Angioedema associated with angiotensin receptor
blockers (ARB’s) has been occasionally reported and
hence their use in individuals with ACE inhibitor-
related angioedema has been questioned but is not con-
tra-indicated [45]. The patient usually presents with
swelling of the tongue, but the lips, pharynx, larynx
and viscera may also be involved. Fatalities are
reported [46], and hence, it is mandatory to recommend
that the ACE inhibitor is withdrawn. The episodes of
angioedema may persist for several months after with-
drawal of the ACE inhibitor without undermining the
validity of the drug-related diagnosis [45]. Individuals
of Afro-Caribbean origin are at increased risk of ACE
inhibitor-induced angioedema. As this group of drugs
are less effective in such individuals, an alternative
choice of antihypertensive is prudent [42, 43, 47]. Anti-
histamines, corticosteroids and adrenaline have tradi-
tionally been used to treat these individuals although
their efficacy remains unproven. However, bradykinin
antagonists, such as icatibant, may be effective. These
drugs are undergoing clinical trials and may prove use-
ful. C1 inhibitor concentrate is not beneficial in patients
with acute angioedema associated with ACE inhibitors.
Follow-up studies on individuals with presumed ACE
inhibitor-related angioedema show that in the majority
symptoms disappear or are drastically reduced after
stopping the ACE inhibitor. Individuals who do not
improve even after several months of stopping the ACE
inhibitor are likely to have an alternative explanation
for their angioedema and were coincidentally taking an
ACE inhibitor. There are no routine investigations to
distinguish responders from non-responders to ACE
inhibitor withdrawal. If the ACE inhibitor is responsible
but is not withdrawn, the attacks may become more
severe and frequent. ACE inhibitors are contraindicated
in patients with a history of angioedema and an alter-
native antihypertensive should be substituted.
Hereditary angioedema (HAE). Angioedema occurs
without weals in HAE and typically involves cutaneous
sites, gut and larynx. A family history should be
sought. HAE can be subdivided into three types. Types I
and II are caused by mutations of the SERPING1 gene
and are associated with deficient levels of C1 inhibitor
or a dysfunctional C1 inhibitor, respectively. Type III is
associated with mutations of Factor XII and the levels
of C1 inhibitor remain normal or only slightly reduced.
These mutations appear to be markers of enhanced ki-
nin production. Type III affec ts women more frequently
and more severely, probably related to the effect of oes-
trogen in promoting angioedema [48]. The benefit of
progestin contraception rather than an oestrogen–pro-
gestin contraception in Type III is reported [49]. Com-
bined oral contraception should be avoided in all
women with HAE [50].
Prognosis
At least 20% of chronic urticaria patients with symp-
toms severe enough to warrant hospital referral remain
symptomatic 10 years after first presentation and this
compares closely with a study published a decade ear-
lier [51, 52]. Increased duration of chronic urticaria cor-
relates with clinical severity, the presence of
angioedema and positive antithyroid antibodies [53]. A
positive autolo gous serum test has been correlated with
more severe symptoms but not prolong ed disease dura-
tion [7, 13].
Making the diagnosis
Clinical history and examination. A detailed history of
urticaria and angioedema is essential and should fully
document the frequency, circumstances of onset, trig-
gers, timin g, pattern of recurrence and duration of
attacks. The history and examination should also
include a description of the nature, site and duration of
individual lesions and whether they itch or are painful.
Photographs of urticaria and angioedema can be helpful
in confirming the nature of the lesions. Detailed drug
and family history as well as response to treatment are
important. Important points to be considered when tak-
ing a clinical history are listed in Boxes 2 and 3. The
clinical history often identifies triggers and is essential
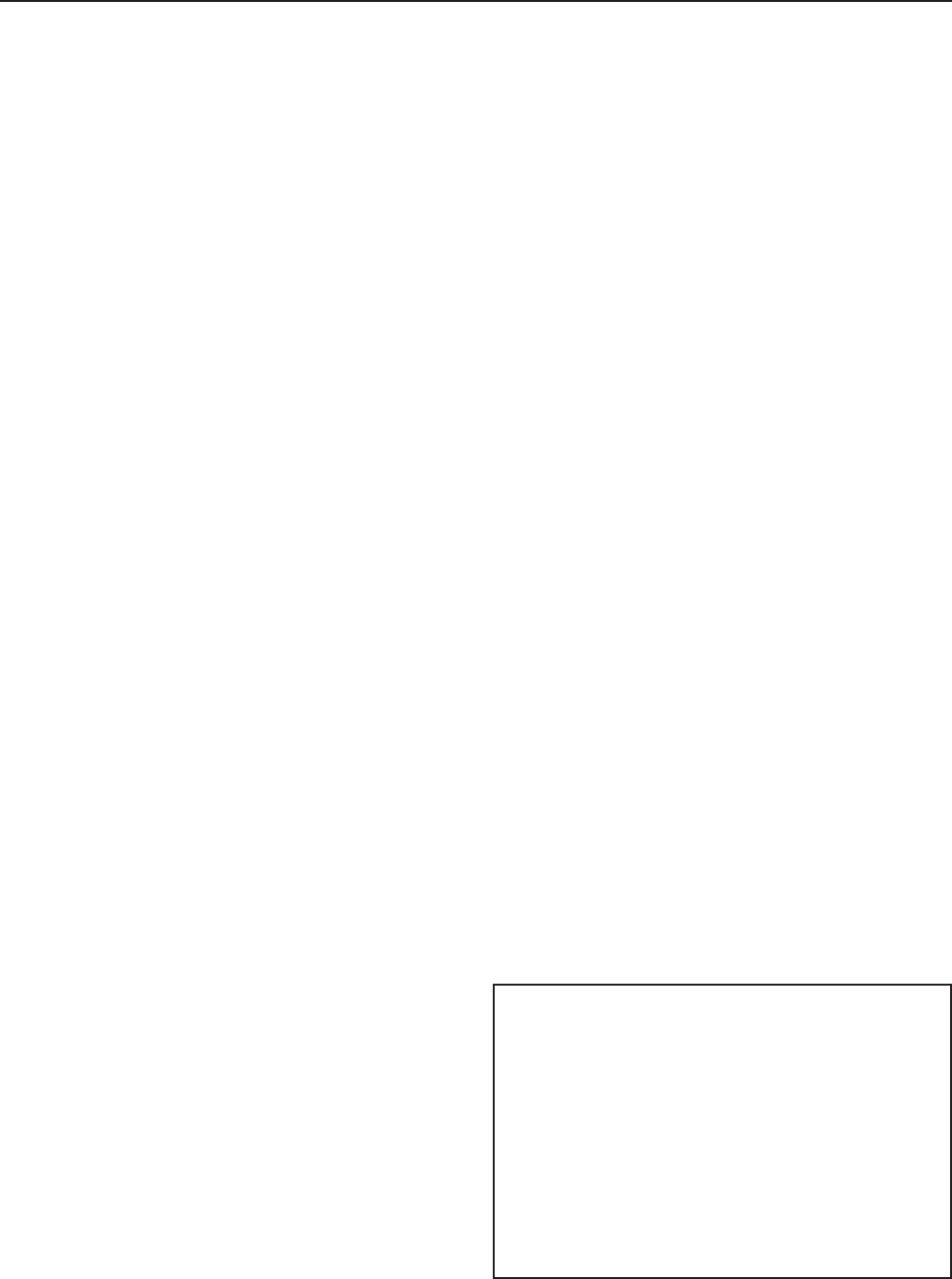
to direct further investigation. Figure 1 shows an
algorithm for the diagnosis of chronic urticaria and/or
angioedema.
Box 2. Questions when considering an ‘allergic’ cause?
•
Could it be related to any drugs the patient has
taken (ACE inhibitor/aspirin/NSAID)?
•
Does it occur only and reproducibly within
60 min (usually within 20 min) of eating a particular
food? Exceptions meat and crustaceans (such as
prawn).
•
Does it occur only if a particular food (e.g. wheat)
has been eaten followed by exercise?
•
Does it occur after contact with an allergen to
which the patient is sensitized (animals, grass, food,
latex, etc.)?
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
552 R. J. Powell et al

Investigations
The diagnosis is based primarily on the clinical presen-
tation. The need for investigations to elucidate a possi-
ble underlying cause should be guided by the
presentation and response to antihistamines (Table 2)
[54].
Allergy testing. Patients are often referred to hosp ital in
the belief that foods are responsible for their chronic
urticaria. A practical approach could be to exclude an
atopic diathesis by skin prick testing (SPT) to a panel of
aeroallergens and suspect foods. The sight of negative
SPTs in certain patients helps to reassure the patient
that allergy is not the cause of their symptoms and may
contribute to improved adherence with long-term anti-
histamines.
When urticaria symptoms are linked to exertion or
exercise, there can be a role for limited specific IgE
testing to related food allergens, e.g. omega-5-gliadin
or lipid transfer proteins [55]. In certain Mediterranean
areas, Anisakis simplex hypersensitivity associated
with the consumption of raw fish should be considered
[56–58].
Full blood count (FBC)—The eosinophil count may be
elevated in parasitic infections and in some drug-
induced reactions. An elevated neutrophil count can be
associated with urticarial vasculitis.
Urinalysis—A screen for haematuria and proteinuria will
help to detect the presence of urinary tract infection
and renal involvement in vasculitis.
Acute phase response—An elevated ESR and/o r CRP
suggests an underlying systemic condition such as
chronic infection, vasculitis and a high ESR with nor-
mal CRP may indicate paraproteinaemia.
Thyroid function and auto-antibodies—The presence of
thyroid auto-antibodies is associated with chronic
URTICARIA
± ANGIOEDEMA
ANGIOEDEMA
Lesions last > 24 hours or
systemic features, e.g. arthralgia
Associated
autoimmune disorder
Exclusion of all known
precipitating factors
On
ACE
inhibitor
Low C4
± low or normal
C1 inhibitor
Low C4
with
paraprotein
Consider other tests
including skin biopsy
as clinically indicated
Urticarial
vasculitis
No vasculitis
Spontaneous
urticaria/angioedema
Consider
delayed-pressure
urticaria
Autoimmune urticaria
possible
Consistent with IgE mediated allergy
trigger, e.g. latex, animal, food
On a drug
known to cause or aggravate
urticaria +/– angioedema
Hereditary
angioedema
Acquired C1
esterase inhibitor
deficiency
(Acquired
angioedema)
Further appropriate tests
negative
Drug-induced urticaria
and/or angioedema
Probably drug
associated
STOP ACE inhibitor
Consider trial
off drug
Fig. 1. Algorithm for diagnosis of chronic urticaria and/or angioedema.
Box 3. Is there a vasculitic process?
•
Are the episodes of urticaria/angioedema persis-
tent rather than evanescent and self-limiting?
•
Do individual lesions last more than 24 h?
•
Are the urticarial lesions tender and painful
rather than itchy?
•
Does the skin sh ow evidence of residual petechial
haemorrhage, purpura or bruising?
•
Does the patient have any symptoms and signs of
underlying disease, e.g. fever, significant malaise,
arthralgia, hypertension, and blood or protein in
urine?
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 553

urticaria in both children and adults and suggests a
diagnosis of autoimmune urticaria. Such patients are
often euthyroid but require monitoring over time. Thy-
roxine treatment is not indicated in euthyroid individu-
als with CU and thyroid autoimmunity [59].
Approximately 20% of patients with chronic urticaria
have antithyroid antibodies [60–62] compared to 6% in
the general population [60].
Complement studies—C1 inhibitor deficiency is not asso-
ciated with urticaria, and hence, if urticaria is present,
measurement of C1 inhibitor is not required. Initial
complement investigations in patients with angioedema
without weals should include C4 and C1 inhibitor. The
C4 level will be low in most cases of Types I and II
HAE even between attacks. Functional C1 inhibitor
quantitation should be reserved for equivocal cases with
a suggestive history and low C4 but normal levels of
antigenic C1 inhibitor [63]. C3 and C4 should be mea-
sured in individuals with suspected urticarial vasculitis
[53], and if reduced, measurement of anti-C1q antibod-
ies may be useful.
Haematinics and vitamins—If clinically indicated, mea-
surement of serum iron [64] and vitamin B12 [65] lev-
els can be useful.
Immunoglobulins—Individuals, usually older than
40 years with CU and systemic symptoms such as one
of the following: malaise, fever, polyarthralgia, lymph-
adenopathy, leukocytosis, should have serum immuno-
globulins and electrophoresis undertaken to search for
an IgM paraprotein that may be ind icative of Schnitzler
syndrome [66]. Cryoglobulins can be associated with
secondary cold urticaria (requires a clotted sample col-
lected and transported to the laboratory at 37°C).
Acquired angioedema without urticaria can be associ-
ated with a B cell lymphoma and a search for a para-
protein may be indicated.
Parasitology—A clear association between parasitaemia
and CU has not been established.
Challenges—Cold-induced urticaria can usually be diag-
nosed by placing an ice cube in a sealed plastic bag
over the forearm for up to 10 min (allow skin to
rewarm subsequently). Dermographism is suspected at
the time of skin prick testing and confirmed by lightly
scratching the skin with weals appearing within
10 min. The water test for aquagenic urticaria may be
applied by immersion of a body part into water (at
37°C) or by placing wet towels for a few minutes onto
the area of skin most affected. Cholinergic urticaria is
triggered by sweating due to heat, emotion or exercise
and can be provoked by exercising the patient in a
warm environment although this is not routinely under-
taken.
Skin biopsy—A lesional skin biopsy is appropriate when
there is an unusual pattern of presentation or in cases
of suspected vasculitis. Clinical clues include systemic
symptoms (fever and arthralgia or arthritis) and lesions
lasting for more than 24 h, or associated with tender-
ness, petechiae, purpura or skin staining as the lesions
fade. Linear bruising suggests excessive scratching
[11].
Autologous serum skin test and basophil release assay—
These both remain research tools. The autologous
serum skin test (ASST) involves intradermal injection
of the patient’s own serum. A positive weal and flare
reaction is considered indicative of circulating auto-
antibodies to the high-affinity IgE receptor on the mast
cell in CU patients [67]. The ASST is poorly tolerated
by younger children due to the discomfort associated
with intraderma l injections performed in the absence
of topical anaesthetic creams [18]. The role of the
basophil histamine release assay (BRA) in the clinical
management of CU remains unclear. The available
assays (BRA and ASST) for autoimmunity in CU do
not consistently assist clinicians in their understanding
of spontaneous CU pathogen esis [68] and remain
research tools.
Nasendoscopy—Nasendoscopy can be considered in an
individual with unexplained pharyngeal obstruction,
and this can be very useful during an attac k allowing
direct visualization of the pharynx/larynx to establish
or exclude the presence of angioedema of the throat.
Important differential diagnoses of ‘swelling, lump or
discomfort in the throat’ include globus, gastro-oesoph-
ageal reflux and vocal cord dysfunction.
Treatment in adults
Avoidance strategies. Symptom diaries can be useful as
an investigative tool to determine the frequency,
duration and severity of the urticarial episodes and
disease-specific QoL questionnaires /symptom scores are
available [69, 70]. Patients who fail to uncover a con-
sistent trigger are advised to discontinue the search for
an external cause.
If avoidable triggers (Table 1) are identified, the
patient should be given clear instructions on avoidance
strategies, for example avoiding cold or pressure. If the
patient is taking a drug associated with chronic urti-
caria or ang ioedema, for example a NSAID, it is pru-
dent for the patient to have a trial for at least several
weeks without this treatment. ACE inhibitors are con-
traindicated in angioedema regardless of the presence
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
554 R. J. Powell et al

or absence of weals. Treatment of underlying infections
and malignancies may lead to amelioration or resolu-
tion of symptoms. Alcohol can aggravate CU by its
effect of vasodilation [71].
Symptom control. In many cases, treatment of CSU is
predominantly directed towards symptom control and
therefore antihistamines active against the H1 receptor
remain the mainstay of treatment. Second-generation
antihistamines are commonly prescribed and are gener-
ally well tolerated with minimal sedation: many have a
once-daily dosage to improve adherence (see Table 4).
Pharmacokinetics suggest that to rapidly achieve opti-
mal blood levels and hence rapid relief of symptoms,
two tablets of the chosen antihistamine m ay be taken
as the first dose, reverting to a single daily tablet there-
after. Studies of higher dose non-sedating antihista-
mines demonstrate efficacy with up to 49 the
conventional dose using levocetirizine or desloratadine
[72]. Once symptom control has been accomplished,
daily treatment [73] is advised in m ost patients for 3–
6 months. For individuals with a long history at presen-
tation of urticaria with angioedema, treatment for 6 or
even 12 months is advised with gradual withdrawal
over a period of weeks. For patients with infrequent
symptoms, treatment may be taken as required or even
prophylactically (e.g. prior to occasions when symptoms
would be most unwelcome, such as business presenta-
tions). Figure 2 shows a step-up treatment plan for
chronic urticaria. A short course of corticosteroids may
be appropriate in severe episodes at any stage (e.g.
prednisolone up to 40 mg daily for 7 days) [74].
Patient-reported outcomes are available for the evalua-
tion of urticaria patie nts [75].
Standard treatment. Choice of H1-antihistamine—All
antihistamines are licensed for use in chronic urticaria,
but the chronic use of first-generation antihistamines,
such as chlorphenamine, should be avoided where pos-
sible because of sedation and interference with psycho-
motor performance. Sedation and impaired
psychomotor function is reduced with seco nd-genera-
tion antihistamines, it but can still occur. Although a
sedating antihistamine at night can sometimes be use-
ful, the long half-life of hydroxyzine can cause day-
time somnolence [76]. Additional anti-inflammatory
effects as suggested by the various antihistamine man-
ufacturers may be relevant to the treatment of chronic
urticaria, but the impact on clinical practice has not
been quantified [77]. Table 3 lists the antihistamines
(H1-antihistamines) ind icated for use in chronic urti-
caria.
The efficacy of the various antihistamines using sup-
pression of the weal and flare response does not corre-
late with clinical urticarial responses and hence should
not be solely used to predict or compare clinical
responses in CU [78–80].
The absence of head to head comp arisons in clinical
trials prevents stratification of efficacy. Table 3 lists
the antihistamines (H1-antihistamines) indicated for
use in chronic urticaria. Individual patient responses
and side-effects to antihistamines vary and an
endorsement for a particular antihistamine cannot be
given. If higher than recomme nded doses of antihista-
mines are to be considered, incremental updosing is
advised.
Tranexamic acid—Tranexamic acid appears to benefit
patients with angioedema particularly those without
weals and inhibits the conversion of plasminogen to
plasmin and consequently the production of bradykinin.
The evidence is anecdotal, but common usage recom-
mends consideration in problematic cases.
Refractory treatment. In cases of chronic urticaria and
angioedema, resistant to high-dose antihistamines, there
is no recommended second-line therapy, but the treat-
ment options given in Tables 4 and 5 and Fig. 2 may
be considered depending on the presenting clinical
symptoms, specific trigger factors and underlying
pathology.
Leukotriene receptor ant agonists—Leukotriene receptor
antagonists may be useful in combination with antihis-
tamines in a subgroup of patients with chronic urti-
caria, particularly those with adverse responses to
aspirin, NSAIDs and in those with delayed press ure urti -
IDENTIFICATION OF TRIGGERS
EDUCATION AND AVOIDANCE OF TRIGGERS
1) Standard dose non-sedating H1 antihistamine
2) Higher dose of H1-antihistamine up to four times
recommended dose or add in second antihistamine
3) Consider a second line agent, anti-leukotriene or, if
angioedema is present, use tranexamic acid
4) Consider an immunomodulant (e.g.
omalizumab, cyclosporine
Fig. 2. General management plan for chronic urticaria (Adults and
children). The starting point and the rate of progression between steps
depend on clinical severity and response. Short course of corticoster-
oids (e.g. 1 mg/kg prednisolone twice a day, up to 40 mg total per
day, for 3 days) may be used for severe exacerbations [74, 146], see
also section on rescue medication. The treatment should be stepped
down once control is achieved. Observations on the mechanism of
antihistamine action [147] suggest that it is probably sensible to with-
draw such therapy gradually, rather than stopping it abruptly.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 555

caria or CaU [81–85]. See also evidence Table B3
(Appendix).
Anti-IgE therapy—Omalizumab is effective in random-
ized double-blind placebo-controlled trials in patients
with spontaneous and autoimmune CU who have per-
sistent symptoms despite high- dose antihistamines [86].
An EAACI position paper recommends omalizumab
when higher dose antihistamines have failed [74]. It
requires monthly injections and appears well tolerated.
It is effective in approximately 80% of individuals with
persistent/resistant symptoms leading to a rapid
improvement. Currently, treatment is recommended for
6 months, but typically relapses occur when treatment
is discontinued.
Ciclosporin—Low-dose ciclosporin may also be consid-
ered in patients with severe unremitting disease uncon-
trolled by antihistamines [87, 88]. A T cell-mediated
mechanism has been proposed, but ciclosporin also
Dose Licensed dose Other comments/side-effects References
Acrivastine 8 mg tds Second-generation antihistamine
Rapid onset of action, not long-lasting,
excreted unchanged in urine;
non-sedating; ‘on-demand’ therapy
[97]
Bilastine 20 mg Second-generation antihistamine [120]
Cetirizine 10 mg Second-generation antihistamine [84, 85, 87, 121]
Chlorphenamine 4 mg qds First-generation antihistamine
Not for long-term use; injectable;
short half-life; sedating
Desloratadine 5 mg Second-generation antihistamine [81, 82, 122]
Fexofenadine 120–180 mg Second-generation antihistamine [83, 101, 123]
Hydroxyzine 25 mg–100 mg
daily
First-generation antihistamine
Not for long-term use; sedating
Levocetirizine 5 mg Second-generation antihistamine [71]
Loratadine 10 mg Second-generation antihistamine [124, 125]
Mizolastine 10 mg Second-generation antihistamine [126]
Promethazine 10–20 mg tds First-generation antihistamine
Not for long-term use, injectable;
sedating
T. Dean, personal
communication
Rupatadine 10 mg Second-generation antihistamine [127]
None of the above second-generation antihistamines has demonstrated superiority over another
in licensed doses. The effectiveness of levocetirizine and desloratadine in up to four times the
conventional doses has been demonstrated in difficult to treat urticaria [72].
Table 3. Antihistamine (H1-antihistamines)
licensed for CU
Table 4. Second-line pharmacotherapy
Drug (families) Grade Specific indication/comments/side-effects Reference
Omalizumab A Used for chronic urticaria failed on higher
dose antihistamines
[86]
Leukotriene receptor
antagonists (montelukast
1
,
zafirlukast)
B
1
Most effective in combination with antihistamines
Autoimmune urticaria; chronic urticaria with
positive challenge to food, food additives or aspirin;
delayed pressure urticaria
[81–83, 122, 128]
Table B3 (Appendix)
Tranexamic acid D Showed reduced frequency of angioedema attacks. [129, 130]
Ciclosporin B Immunosuppresive, i.e. requires monitoring of blood
pressure, renal function and serum levels if indicated;
significant side-effects
[87, 88]
Table B4 (Appendix)
Mycophenolate Mofetil D Used for chronic urticaria failed on
higher dose antihistamines
[89, 131]
Tacrolimus D Value in severe, steroid-dependent chronic urticaria
needs further randomized controlled studies
[132]
Grade = Grade of recommendation (Table B2) [133, 134]. B
1
= Grade only refers to montelukast, but not to zafirlukast.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
556 R. J. Powell et al

inhibits basophil and mast cell degranulation. See also
evidence Table B4 (Appendix).
Mycophenolate mofetil—Open-label studies suggest that
1000 mg twice daily is useful; however, its speed of
onset is slower than with both, omalizumab and ciclo-
sporin [89].
H2-Antihistamines—A recent review [90] concluded that
the evidence for the use of H2-antihistamines in urticaria
was weak. The combination of cimetidine with hydroxy-
zine results in an increased serum level of hydroxyzine
confirming the rationale for its co-administration with
hydroxyzine in some patients with CU unresponsive to
hydroxyzine alone. There is no therapeutic rationale for
co-administration of cimetidine with cetirizine in CU
[91]. In CU, the combination of ranitidine with terfena-
dine was superior to terfenadine alone in terms of itch,
but there was no significant effect on weals or swellings
[92]. There is no strong evidence to support the addition
of ranitidine to treatment regimes in CU.
Rescue medication. Corticosteroids—There are no con-
trolled studies on the use of corticosteroids in urticaria
and angioedema, but their effectiveness is general ly
accepted. Rarely, a short course of up to 40 mg pred-
nisolone may be prescribed for severe exacerbations of
chronic urticaria, especially when accompanied by an-
gioedema [74]. Corticosteroids may also be considered
when the symptoms remain uncontrolled by antihista-
mines alone or when rapid clinical relief is required.
Urticarial vasculitis is more likely to require corticoste-
roid treatment. Longer term corticosteroid usage should
be avoided whenever possible but if unavoidable, the
lowest dose should be adopted. Topical steroids have no
place in the treatment of chronic urticaria.
Intramuscular adrenaline—Self-administered intramus-
cular adrenaline may be indicated in patients with a his-
tory of severe angioedema affecting the upper airway or
urticaria with significant cardiovascular symptoms. In
these individuals, all possible underlying causes should
be investigated and treated appropriately using the step-
up treat ment schedule (Fig. 2) in an attempt to suppress
the oropharyngeal swellings completely. Adrenaline is
not indicated in non-histaminergic angioedema as seen
in HAE and with ACE inhibitors.
Icatibant and CI inhibitor—The therapeutic benefit of i-
catibant and C1 inhibitor in acute attacks of HAE is
recognized [93, 94]. It has been reported in a case series
that icatibant may have efficacy in angioedema induced
by ACE inhibitors [95].
Others. Topical preparations—Cooling antipruritic
lotions such as 2% menthol in aqueous cream can be
soothing [71]. Topical steroids should not be used to
treat chronic urticaria.
Dietary advice—Diets low in salicyl ates and benzoates
have been anecdotally adopted in the management of
Table 5. Rarely used drugs
Drug (families) Grade Specific indication/comments/side-effects Reference
Bradykinin B2 receptor
antagonist (icatibant)
B Licensed for acute attacks of HAE [93, 95]
Dapsone D Several single-case reports of successful
treatments of urticarial vasculitis in resistant cases
Helped one patient with autoimmune thyroiditis
to stop oral steroid treatment
[135–137]
Hydroxy-chloroquine D Improvement of QoL, but no reduction in urticaria
scores or medication requirements
[138]
Methotrexate D Beneficial for corticosteroid-dependent chronic
spontaneous urticaria (2 patients)
Efficacy in urticarial vasculitis (one patient)
[139, 140]
Stanozolol (Danazol) C Beneficial effects in patients with refractory CIU
(with simultaneous cetirizine dose); Long-term effects
unknown; drug currently not licensed, but available
on a named-patient basis as winstrol, 4 mg in the
United Kingdom. Danazol likely to have similar effects
[141]
Sulfasalazine D Successful in 2 patients with refractory delayed pressure
urticaria and angioedema. One was steroid-dependent
and managed to come off prednisolone
[142–144]
Warfarin C Improvement in 6 of 8 patients who were unresponsive
to antihistamines
[145]
Grade = Grade of recommendation (Table B2) [133, 134].
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 557

urticaria. However, there is no evidence to support the
routine use of low salicylate diets [96]. Individuals with
chronic urticaria associated with salicylates may respond
to leukotriene receptor antagonists [82]. Suspected tartr-
azine-induced urticaria/angioedema is rarely reproduc-
ible by oral challenge, and hence, additive-free diets are
not justified in patien ts with CsU [97]. High-dose supple-
mental vitamin D
3
has been re ported to be beneficial irre-
spective of a patient’s vitamin D status. [98].
Psychological interventions—A recent meta-analysis
confirmed the high prevalence of an association
between psychological factors and CU [15]. Even if psy-
chological symptoms develop subsequent to CU and
play little part in its pathogenesis, the positive correla-
tion between CU and markers of poor psy chological
wellness indicates that psychotherapeutic treatments
and behavioural interventions may prove beneficial.
Patient leaflets—See appendices A1 (Adults) and A2
(children).
Chronic urticaria in childhood
Introduction
Chronic urticaria is less common in children than it is
in adults. Up to 40% of children with chronic urticaria
have autoreactive urticaria. There is no difference in
medication requirements or remission rates between
children who are ASST positive or negative. Cold and
pressure urticar ia are the most commonly diagnosed
induced urticarias in children. These may occur in com-
bination with dermographism or cholinergic urticaria.
Chronic spontaneous urticaria in childhood is rarely a
severe disease and usually remits over time. The major-
ity of children will respond to treatment with antihista-
mines and avoidance of triggers [99].
Box 4. Management of adult patients with weals
•
Check that symptomatic episodes have not fol-
lowed ingestion of a non-steroidal anti-inflammatory
drug such as aspirin or ibuprofen.
•
Give explanation of the symptoms and reassur-
ance that the histamine-induced chronic urticaria
symptoms do not involve the respiratory tract (upper
and/or lower) or cardiovascular system – as occurs
in anaphylaxis. There are, however, very rare excep-
tions to this rule.
•
Give a once-daily dose of a long acting, non-
sedating antihistamine (prn, if symptoms are infre-
quent).
•
If necessary, double the dose of antihistamine
(usually given at night), and/or add a second antihis-
tamine.
•
Consider further increase in dose of antihistamine
up to 49 recommended dose.
•
Consider adding one or more second-line drugs
(see Table 4 and Fig. 2).
•
Consider short-term oral corticosteroid rescue
treatment.
Box 6. Management plan for patients with angioedema
without weals in adults
1 Exclude C1 inhibitor deficiency – a norma l plasma
C4 during an attack, or normal C4, C1 inhibitor,
and C1 inhibitor function, between attacks, will
typically exclude this.
2 If the patient is taking an ACE inhibitor, this drug
should be stopped.
3 Even if the patient is not taking an ACE inhibitor,
these drugs should be avoided in the future.
4 Give a once-daily dose of a long acting, non-sedat-
ing antihistamine (prn, if symptoms are infrequent)
and consider higher doses of antihistamines.
5 Consider tranexamic acid in antihistamine-resis-
tant angioedema.
6 An adrenaline auto-injector and short-term oral
corticosteroids are unlikely to be beneficial unless
an underlying histaminergic mechanism is consid-
ered to be responsible for the angioedema.
Box 5. Management plan for patients with angioedema
with weals in adults
In addition to instructions in ‘Box 4’ above, the
following steps should be considered:
1 If the patient is taking an ACE inhibitor, this drug
should be stopped.
2 Even if the patient is not taking an ACE inhibitor,
these drugs should be avoided in the future.
3 Consider addition of tranexamic acid for higher
dose antihistamine-resistant angioedema.
4 An adrenaline auto-injector is rarely required and
should only be considered if there is a history of
significant angioedema affecting the upper airway
(rare in angioedema with urticaria). The patient
should then be shown how to use the device and
provided with a written self-management protocol.
5 Consider short-term oral corticosteroid rescue
treatment.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
558 R. J. Powell et al

Acute spontaneous urticaria is not covered in this
guideline, although it remains the commonest form of
urticaria in childhood. In atopic children, acute urticaria
may occur as part of an allergic reaction, e.g. to food. If so,
it usually develops within an hour of eating the food and
resolves within 24 h. Acute spontaneous urticaria may
also occur in response to a viral infection, when it usually
persists for longer than 24 h and may last several days.
Epidemiology and clinical presentation
Urticaria (acute, intermittent and chronic ) affects
around 3.4% of British children. Only a small propor-
tion of these are chronic [100]. Approximately 50–80%
of children with chronic urticaria have associated an-
gioedema [11]. Chronic urticaria/angi oedema in child-
hood is usually not life-threatening. Concerns about the
physical appearance of weals and angioedema and
associated systemic symptoms may combine to impair
quality of life. It is not uncommon for children to have
missed significant periods of school, due to a lay per-
ception that their appearance is infectious or allergic
and fear that the child is ‘unwell’.
Aetiology and mechani sms
Investigations are rarely required in children presenting
with chronic urticaria. A detailed clinical history and
physical examination usually establishes the diagnosis.
Most are spontaneous with physical factors such as
pressure or cold exposure being the most commonly
diagnosed precipitating factors. 31–47% of children
with CU have an autoimmune aetiolo gy with a positive
ASST [18, 19]. About 4% of children with CU have
positive antithyroid antibodies, the majority of these
are euthyroid [101 ] (Table 2).
Vasculitides and connective-tissue disorders. The com-
monest ca use of acute vasculitic urticaria in children is
Henoch–Schonlein purpura. This is a clinical diagnosis
presenting with a distinctive rash over the extensor sur-
faces of the legs and buttocks [102]. Rare causes of
chronic urticaria should be considered in patients with
other systemic symptoms or raised inflammatory mark-
ers [103]. A diagnostic lesional skin biopsy could be
considered if features such as fever, painful lesions,
arthralgia, raised ESR, lesions lasting 24 h or more or
lesions that resolve revealing purpura or petechiae.
Thyroid autoimmunity. An association between child-
hood chronic urticaria and thyroid autoimmunity has
been postulated [101, 104]. It is not clear whether the
association is causal, as the majority of children present
with hyper- or hypothyroid symptoms either before or
some time after the onset of chronic urticaria. The urti-
carial symptoms do not always improve with thyroxine
replacement therapy. Nonetheless, ongoing thyroid
function monitoring is encouraged for children with CU
and thyroid autoimmunity [18, 101].
Coeliac disease. There are case reports of an association
between chronic urticaria and coeliac disease, which
may improve on a gluten-free diet [105, 106].
Prognosis
Parents need reassurance that this is not a severe dis-
ease and that it remits over time. A quarter of children
with chronic spontaneous urticaria are disease-free
3 years after presentation [18], and 96% are asymptom-
atic after 7 years. Children with physical urticarias
should be advised to avoid triggers and the condition
usually regresses spontaneously after 2–3 years.
Investigations
A detailed clinical history is extremely important for
any decisions regarding further investigations. If the
clinical history and examination are typical of CsU,
then further laboratory investigations are rarely useful.
Chronic urticaria is commonly perceived by the parents
to be due to an allergic or idiosyncratic reaction to
foods or food additives, such as food preservatives or
food dyes. There is little published evidence to support
this. Families often find it helpful to see a lack of atopy
demonstrated by negative skin tests.
Skin tests/specific IgE testing. If the clinical history
suggests a candidate allergen, then allergy tests (skin
testing or specific IgE tests) are warranted. The range of
allergens tested should be guided by the history to
avoid the need to explain any false-positive results.
Additional investigat ions if clinically indicated.
•
Urinalysis
•
Full blood count (FBC)
•
Erythrocyte sedimentation rate (ESR)
•
Liver function tests (add viral hepatitis screen if
transaminases are abnormal)
•
Coeliac screen: Tissue transglutaminase IgA antibod-
ies and/or endomysial IgA antibodies – if abnormal or
history suggestive, refer for intestinal biopsy. If the
patient is on a gluten-free diet or has IgA deficiency,
these tests may be misleading
•
Thyroid function and antithyroid antibodies
•
Cold, dermographism and pressure provocation tests
[107]
•
Elimination rechallenge diets: rarely, it may be nec-
essary to undertake carefully planned and dietician-
supervised elimination and rechallenge diets
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 559

•
Antinuclear antibodies should only be measured if a
connective-tissue disorder is clinically suspected
•
A skin biopsy may be indicated if vasculitis is sus-
pected
•
C4 and C1 inhibitor quantitation to detect C1 inhibi-
tor deficiency are only indicated for children, typically
teenagers, presenting with angioedema without urticaria
to define the presence or absence of C1 inhibitor defi-
ciency [108]
•
Tests for current or past viral, bacterial or parasitic
infections should be guided by the history, clinical
findings and initial screening tests, e.g. eosinophilia
Treatment in children
Management plan. Avoidance of known provoking
stimuli should be the primary strategy in any treatment.
Drug treatment is described in the management plan in
Fig. 2.
H1-antihistamines (grade of recommendation = B)—
Non-sedating antihistamines are the mainstay of treat-
ment for children with chronic urticaria. Up to four
times the recommended dose may be required to ade-
quately contro l symptoms. A lack of response to high-
dose antihistamine therapy should raise the possibility
of an underlying diagnosis such as vasculitis. Chronic
urticaria may present as early as the second year of
life and this can limit the choice of licensed antihista-
mine [18, 19]. Cetirizine and desloratadine are licensed
for the treatment of chronic urticaria in children from
1 year of age; loratadine and levocetirizine are
licensed for the treat ment of children of 2 years and
older. Acrivastine, bilastine, fexofenadine, mizolastine
and rupatadine are licensed for use in children over
12 years. Des loratadine, levocetirizine, loratadine and
cetirizine are available in syrup formulations. The
metabolism of cetirizine in children is different to that
in adults, and hence, this drug should be taken twice
daily.
First-generation sedating antihistamines. Children may
become accustomed to the sedating effects of first-gen-
eration antihistamines; howeve r, the risk of psychomo-
tor impairment remains and this may impact on the
child’s safety and education. Those licensed for use in
childhood include diphenhydramine, hydroxyzine, pro-
methazine and chlorphenamine.
Leukotriene receptor antagonists (grade of recommenda-
tion = C)—Evidence for the effectiveness of leukotriene
receptor antagonists (LTRAs) as monotherapy is poor .
Patients not responding to antihistamines alone should
be offered a 1- to 4-week trial of the addition of a
LTRA, e.g. montelukast 4–10 mg nocte.
Corticosteroids (grade of recommendation = D)—Short-
term use of oral corticosteroids (3–5 days ) may be
required to gain control of symptoms. In inducible urti-
caria unresponsive to first-line therapy, corticosteroids
are poorly effective. In patients with delayed pressure
urticaria, corticosteroids are more effective [100]. Pro-
longed use of oral corticosteroids produces unacc ept-
able/severe side-effects.
Tranexamic acid. Tranexamic acid can be effective in
the treatment of isolated angioedema [109]. A dose of
15–25 mg/kg (maximum 1.5 g) 2–3 times per day is
recommended.
Anti-IgE. There is increasing evidence for the efficacy
and sa fety of Omalizumab in children ove r 7 years of
age with CU, resistant to first-line treatment. Three to
six injections of 150–300 mg are administered monthly
[86, 110, 111]. The tre atment is well tolerated, but
should be restricted to specialist centres.
Other treatments. Other therapies such as ciclosporin
[100, 101] should be limited to use in difficult cases
and only considered in specialist centres.
Chronic urticaria in pregnancy and breastfeeding
Pregnancy. Chronic urticaria often improves in preg-
nancy, reducing the need for antihistamine treatment,
although in some rare cases, urticaria deteriorates. It is
best practice to avoid taking drugs in pregnancy. There
is no evidence in humans that antihistamines are tera-
togenic, but in animal studies using high doses of
hydroxyzine and loratadine have led to embryotoxicity.
The data sheets for cetirizine, desloratadine, hydroxy-
zine and loratadine all advise avoidance in pregnancy.
Hydroxyzine is specifically contraindicated in early
pregnancy.
Pregnant women should be informed that no drug
can be considered absolutely safe, and the benefits of
keeping the mother healthy have to be balanced against
the small risk to the foetus. The consequences of inade-
quately controlled disease should be discussed with the
patient and documented in the case notes.
There is considerable clinical experience with cetiri-
zine and loratadine in pregna ncy, with no increase in
the rate of congenital abnormalities [112–117].
Cetirizine and loratadine have been as signed a cate-
gory B by the US FDA. Hence, antihistamines should
only be used if clearly needed and when the potential
benefits outweigh the unknown risks to the foetus.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
560 R. J. Powell et al

Breastfeeding. Antihistamines should only be used dur-
ing lactation when the clinical imperative outweighs
the potential harm to the child. The lowest dose should
be used for the shortest duration. Significant amounts
of antihistamines are excreted in breast milk and,
although not known to be harmful, the manufacturers
of most antihistamines advise avoidance whilst breast-
feeding. Chlorphenamine may cause drowsiness and
poor feeding. Both loratadine [118] and cetirizine
appear safer with only low levels found in breast milk
[119], and therefore, these drugs could be considered if
required.
Future research – key areas
•
Well-controlled clinical trials in chronic urticaria
that does not respond to standard therapy are required.
Such studies should have the appropriate statistical
power to clarify which drugs should be used, in what
dose and for how long. Studies to investigate whether
the presence of angioedema affects the prognosis of
disease.
•
Investigation of the role of exacerbating factors in
urticaria and angioedema, e.g. NSAIDs, stress.
•
Studies designed to correlate clinical presentation
with prognosis and response to treatment, e.g. the use
of tranexamic acid in spontaneous (idiopathic) angio e-
dema.
•
Studies designed to understand the clinico-patholog-
ical association of thyroid autoimmunity and autoim-
mune urticaria.
•
Development of reliable laboratory assays for identi-
fication of autoimmune urticaria.
•
Systematic review of psychological interventions in
CsU.
This guideline informs the management of urticaria
and angioedema. Adherence to this guideline does not
constitute an automatic defence for negligence and
conversely non-adherence is not indicative of negli-
gence. It is anticipated that this guideline will be
reviewed 5 yearly.
Acknowledgements
The preparation of this document has benefited from
extensive discussions within the Standards of Ca re
Committee of the BSACI and we would like to acknowl-
edge all the members of this committee for their valu-
able contribution, namely Elizabeth Angier, Nicola
Brathwaite, Tina Dixon, Pamela Ewan, Sophie Farooque,
Thirumala Krishna, Rita Mirakian, Helen Smith and Ste-
phen Till. We give special thanks to Clive Grattan for
his invaluable advice. We would also like to thank our
lay advisor, Nicola Mundy, for her valuable comments.
She reviewed a draft of this guideline and her suggested
changes were incorporated into the final document.
Finally, we would like to acknowledge the very valu-
able considerations and criticism we received from
many BSACI members during the consultation process.
Conflict of interests were recorded by the SOCC. None
jeopardized unbiased guideline development.
References
1 Gaig P, Olona M, Munoz LD et al.
Epidemiology of urticaria in Spain.
J Investig Allergol Clin Immunol
2004; 14:214–20.
2 Greaves MW. Chronic idiopathic urti-
caria. Curr Opin Allergy Clin Immunol
2003; 3:363–8.
3 Baiardini I, Giardini A, Pasquali M
et al. Quality of life and patients’ sat-
isfaction in chronic urticaria and
respiratory allergy. Allergy 2003;
58:621–3.
4 Maurer M, Ortonne JP, Zuberbier T.
Chronic urticaria: a patient survey on
quality-of-life, treatment usage and
doctor-patient relation. Allergy 2009;
64:581–8.
5 O’Donnell BF, Lawlor F, Simpson J,
Morgan M, Greaves MW. The impact
of chronic urticaria on the quality of
life. Br J Dermatol 1997; 136:197–
201.
6 Kozel MM, Sabroe RA. Chronic urti-
caria: aetiology, management and
current and future treatment options.
Drugs 2004; 64:2515–36.
7 Sabroe RA, Fiebiger E, Francis DM
et al. Classification of anti-Fcepsi-
lonRI and anti-IgE autoantibodies in
chronic idiopathic urticaria and corre-
lation with disease severity. J Allergy
Clin Immunol 2002; 110:492–9.
8 Kikuchi Y, Kaplan AP. A role for C5a
in augmenting IgG-dependent hista-
mine release from basophils in
chronic urticaria. J Allergy Clin
Immunol 2002; 109:114–8.
9 Zuberbier T, Balke M, Worm M,
Edenharter G, Maurer M. Epidemiol-
ogy of urticaria: a representative
cross-sectional population survey.
Clin Exp Dermatol 2010; 35:869–73.
10 Kikuchi Y, Kaplan AP. Mechanisms of
autoimmune activation of basophils
in chronic urticaria. J Allergy Clin
Immunol 2001; 107:1056–62.
11 Kaplan AP. Clinical practice. Chronic
urticaria and angioedema. N Engl J
Med 2002; 346:175–
9.
12 Vazquez NF, meida Arvizu VM, San-
chez Nuncio HR, Villanueva Carreto
ML, Guidos Fogelbach GA. Prevalence
and potential triggering factors of
chronic urticaria and angioedema in
an urban area of northeastern Mexico.
Rev Alerg Mex 2004; 51:181–8.
13 Sabroe RA, Seed PT, Francis DM, Barr
RM, Black AK, Greaves MW. Chronic
idiopathic urticaria: comparison of
the clinical features of patients with
and without anti-FcepsilonRI or anti-
IgE autoantibodies. J Am Acad Der-
matol 1999; 40:443–50.
14 Ricci G, Giannetti A, Belotti T et al.
Allergy is not the main trigger of
urticaria in children referred to the
emergency room. J Eur Acad Derma-
tol Venereol 2010; 24:1347–8.
15 Ben-Shoshan M, Blinderman I, Raz A.
Psychosocial factors and chronic
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 561

spontaneous urticaria: a systematic
review. Allergy 2013; 68:131–41.
16 Oliver MG, Specian RD, Perry MA,
Granger DN. Morphologic assessment
of leukocyte-endothelial cell interac-
tions in mesenteric venules subjected
to ischemia and reperfusion. Inflam-
mation 1991; 15:331–46.
17 Ley K. Integration of inflammatory
signals by rolling neutrophils. Immu-
nol Rev 2002; 186:8–18.
18 Du Toit G, Prescott R, Lawrence P
et al. Autoantibodies to the high-
affinity IgE receptor in children with
chronic urticaria. Ann Allergy Asthma
Immunol 2006; 96:341–4.
19 Brunetti L, Francavilla R, Miniello VL
et al. High prevalence of autoimmune
urticaria in children with chronic urti-
caria. J Allergy Clin Immunol 2004;
114:922–7.
20 Gruber BL, Baeza ML, Marchese MJ,
Agnello V, Kaplan AP. Prevalence
and functional role of anti-IgE au-
toantibodies in urticarial syndromes. J
Invest Dermatol 1988; 90:213–7.
21 Konstantinou GN, Asero R, Ferrer M
et al. EAACI taskforce position paper:
evidence for autoimmune urticaria
and proposal for defining diagnostic
criteria. Allergy 2013; 68:27–36.
22 Bossi F, Frossi B, Radillo O et al. Mast
cells are critically involved in serum-
mediated vascular leakage in chronic
urticaria beyond high-affinity IgE
receptor stimulation. Allergy 2011;
66:1538–45.
23 Asero R, Tedeschi A, Lorini M, Salim-
beni R, Zanoletti T, Miadonna A.
Chronic urticaria: novel clinical and
serological aspects. Clin Exp Allergy
2001; 31:1105–10.
24 Ferrer M, Nakazawa K, Kaplan AP.
Complement dependence of histamine
release in chronic urticaria. J Allergy
Clin Immunol 1999; 104:169–
72.
25 Reichel M, Mauro TM. Urticaria and
hepatitis C. Lancet 1990; 336:822–3.
26 Kanazawa K, Yaoita H, Tsuda F,
Okamoto H. Hepatitis C virus infec-
tion in patients with urticaria. JAm
Acad Dermatol 1996; 35:195–8.
27 Siddique N, Pereira BN, Hasan AS.
Hepatitis C and urticaria: cause and
effect? Allergy 2004; 59:668.
28 Vaida GA, Goldman MA, Bloch KJ.
Testing for hepatitis B virus in
patients with chronic urticaria and
angioedema. J Allergy Clin Immunol
1983; 72:193–8.
29 Black AK, Lawlor F, Greaves MW.
Consensus meeting on the definition
of physical urticarias and urticarial
vasculitis. Clin Exp Dermatol 1996;
21:424–6.
30 Commins SP, James HR, Kelly LA
et al. The relevance of tick bites
to the production of IgE antibodies
to the mammalian oligosaccharide
galactose-alpha-1,3-galactose. J Aller
gy Clin Immunol 2011; 127:1286–93.
31 Ozkan M, Oflaz SB, Kocaman N et al.
Psychiatric morbidity and quality of
life in patients with chronic idiopathic
urticaria. Ann Allergy Asthma Immu-
nol 2007; 99:29–33.
32 Picardi A, Abeni D. Stressful life
events and skin diseases: disentan-
gling evidence from myth. Psychother
Psychosom 2001; 70:118–36.
33 Staubach P, Dechene M, Metz M
et al. High prevalence of mental dis-
orders and emotional distress in
patients with chronic spontaneous
urticaria. Acta Derm Venereol 2011;
91:557–61.
34 Torresani C, Bellafiore S, De PG.
Chronic urticaria is usually associated
with fibromyalgia syndrome. Acta
Derm Venereol 2009; 89:389–92.
35 Staubach P, Eckhardt-Henn A, Dech-
ene M et al.
Quality of life in patients
with chronic urticaria is differentially
impaired and determined by psychiat-
ric comorbidity. Br J Dermatol 2006;
154:294–8.
36 Chung MC, Symons C, Gilliam J, Ka-
minski ER. Stress, psychiatric co-mor-
bidity and coping in patients with
chronic idiopathic urticaria. Psychol
Health 2010; 25:477–90.
37 Kaplan AP. Chronic urticaria: patho-
genesis and treatment. J Allergy Clin
Immunol 2004; 114:465–74.
38 Campanati A, Gesuita R, Giannoni M
et al. Role of small intestinal
bacterial overgrowth and Helicobact-
er pylori infection in chronic sponta-
neous urticaria: a prospective
analysis. Acta Derm Venereol 2013;
93:161–4.
39 Federman DG, Kirsner RS, Moriarty
JP, Concato J. The effect of antibiotic
therapy for patients infected with He-
licobacter pylori who have chronic
urticaria. J Am Acad Dermatol 2003;
49:861–4.
40 Agostoni A, Cicardi M. Drug-induced
angioedema without urticaria. Drug
Saf 2001; 24:599–606.
41 Lee A. Adverse drug reactions. 2nd
edn. London UK: Pharmaceutical Press,
2006.
42 Kostis JB, Kim HJ, Rusnak J et al.
Incidence and characteristics of an-
gioedema associated with enalapril.
Arch Intern Med 2005; 165:1637–42.
43 Vleeming W, van Amsterdam JG,
Stricker BH, de Wildt DJ. ACE inhibi-
tor-induced angioedema. Incidence,
prevention and management. Drug
Saf 1998; 18:171–88.
44 Guo X, Dick L. Late onset angioten-
sin-converting enzyme induced an-
gioedema: case report and review of
the literature. J Okla State Med Assoc
1999; 92:71–3.
45 Cicardi M, Zingale LC, Bergamaschini
L, Agostoni A. Angioedema associated
with angiotensin-converting enzyme
inhibitor use: outcome after switching
to a different treatment. Arch Intern
Med 2004; 164:910–3.
46 Dean DE, Schultz DL, Powers RH.
Asphyxia due to angiotensin convert-
ing enzyme (ACE) inhibitor mediated
angioedema of the tongue during the
treatment of hypertensive heart dis-
ease. J Forensic Sci 2001; 46:1239–43.
47 Pavletic AJ. Late angio-oedema in
patients taking angiotensin-convert-
ing-enzyme inhibitors. Lancet 2002;
360:493–4.
48 Longhurst HJ. Hereditary and other
orphan angioedemas: a new prophy-
lactic option at last? Clin Exp Allergy
2013; 43:380–2.
49 Saule C, Boccon-Gibod I, Fain O et al.
Benefits of progestin contraception in
non-allergic angioedema. Clin Exp
Allergy 2013; 43:475–82.
50 Geng B, Riedl MA. HAE update: spe-
cial considerations in the female
patient with hereditary angioedema.
Allergy Asthma Proc 2013; 34:13–8.
51 Humphreys F, Hunter JA. The charac-
teristics of urticaria in 390 patients.
Br J Dermatol 1998; 138:635–8.
52 Champion RH. Urticaria: then and
now. Br J Dermatol 1988; 119:427–36.
53 Toubi E, Kessel A, Avshovich N et al.
Clinical and laboratory parameters in
predicting chronic urticaria duration:
a prospective study of 139 patients.
Allergy 2004; 59:869–73.
54 Kozel MM, Mekkes JR, Bossuyt PM,
Bos JD. The effectiveness of a history-
based diagnostic approach in chronic
urticaria and angioedema. Arch
Dermatol 1998; 134:1575–80.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
562 R. J. Powell et al

55 Gamboa PM, Gonzalez C, Pereira C
et al. Unlocking the resistance to
wheat lipid transfer protein. J Allergy
Clin Immunol 2013; 132:1257–8.
56 Ventura MT, Napolitano S, Menga R,
Cecere R, Asero R. Anisakis simplex
hypersensitivity is associated with
chronic urticaria in endemic areas. Int
Arch Allergy Immunol 2013;
160:297–300.
57 Daschner A, Rodero M, De FC, Valls
A, Cuellar C. Chronic urticaria is asso-
ciated with a differential helminth-
arthropod-related atopy phenotype. J
Dermatol 2010; 37:780–5.
58 Daschner A, De FC, Valls A, Vega F.
Anisakis simplex sensitization-associ-
ated urticaria: short-lived immediate
type or prolonged acute urticaria.
Arch Dermatol Res 2010; 302:625–9.
59 Kiyici S, Gul OO, Baskan EB et al.
Effect of levothyroxine treatment on
clinical symptoms and serum cytokine
levels in euthyroid patients with
chronic idiopathic urticaria and thy-
roid autoimmunity. Clin Exp Dermatol
2010; 35:603–7.
60 Leznoff A, Sussman GL. Syndrome of
idiopathic chronic urticaria and
angioedema with thyroid autoimmu-
nity: a study of 90 patients. J Allergy
Clin Immunol 1989; 84:66–71.
61 Leznoff A, Josse RG, Denburg J, Dolo-
vich J. Association of chronic urti-
caria and angioedema with thyroid
autoimmunity. Arch Dermatol 1983;
119:636–40.
62 Rumbyrt JS, Katz JL, Schocket AL.
Resolution of chronic urticaria in
patients with thyroid autoimmunity. J
Allergy Clin Immunol 1995; 96:901– 5.
63 Gompels MM, Lock RJ, Abinun M
et al. C1 inhibitor deficiency: consen-
sus document. Clin Exp Immunol
2005; 139:379–94.
64 Guarneri F, Guarneri C, Cannavo SP.
Oral iron therapy and chronic idio-
pathic urticaria: sideropenic urticaria?
Dermatol Ther 2014; 27:223–6.
65 Mete N, Gulbahar O, Aydin A, Sin
AZ, Kokuludag A, Sebik F. Low B12
levels in chronic idiopathic urticaria.
J Investig Allergol Clin Immunol
2004; 14:292–9.
66 Simon A, Asli B, Braun-Falco M et al.
Schnitzler’s syndrome: diagnosis,
treatment, and follow-up. Allergy
2013; 68:562–8.
67 Sabroe RA, Grattan CE, Francis DM,
Barr RM, Kobza BA, Greaves MW.
The autologous serum skin test: a
screening test for autoantibodies in
chronic idiopathic urticaria. Br J Der-
matol 1999; 140:446–52.
68 Eckman JA, Hamilton RG, Saini SS.
Independent evaluation of a commer-
cial test for “autoimmune” urticaria in
normal and chronic urticaria subjects.
J Invest Dermatol 2009; 129:1584–6.
69 Mlynek A, Zalewska-Janowska A,
Martus P, Staubach P, Zuberbier T,
Maurer M. How to assess disease
activity in patients with chronic urti-
caria? Allergy 2008; 63:777–80.
70 Jariwala SP, Moday H, de Asis ML
et al. The Urticaria Severity Score: a
sensitive questionnaire/index for
monitoring response to therapy in
patients with chronic urticaria. Ann
Allergy Asthma Immunol 2009;
102:475–82.
71 Grattan C, Powell S, Humphreys F.
Management and diagnostic guide-
lines for urticaria and angio-oedema.
Br J Dermatol 2001; 144:708–14.
72 Staevska M, Popov TA, Kralimarkova
T et al. The effectiveness of levocetiri-
zine and desloratadine in up to 4
times conventional doses in difficult-
to-treat urticaria. J Allergy Clin
Immunol 2010; 125:676–82.
73 Grob JJ, Auquier P, Dreyfus I, Ortonne
JP. How to prescribe antihistamines for
chronic idiopathic urticaria: deslorata-
dine daily vs PRN and quality of life.
Allergy 2009; 64:605–12.
74 Zuberbier T, Aberer W, Asero R et al.
The EAACI/GA(2) LEN/EDF/WAO
Guideline for the definition, classifi-
cation, diagnosis, and management of
urticaria: the 2013 revision and
update. Allergy 2014; 69:868–87.
75 Baiardini I, Braido F, Bindslev-Jensen
C et al.
Recommendations for assessing
patient-reported outcomes and health-
related quality of life in patients with
urticaria: a GA(2) LEN taskforce posi-
tion paper. Allergy 2011; 66:840–4.
76 Staevska M, Gugutkova M, Lazarova
C et al. Night-time sedating H1-anti-
histamine increases daytime somno-
lence but not treatment efficacy in
chronic spontaneous urticaria: a ran-
domized controlled trial. Br J Derma-
tol 2014; 171:148–54.
77 Simons FE. Advances in H1-antihista-
mines. N Engl J Med 2004;
351:2203–17.
78 Monroe EW, Daly AF, Shalhoub RF.
Appraisal of the validity of hista-
mine-induced wheal and flare to pre-
dict the clinical efficacy of
antihistamines. J Allergy Clin Immu-
nol 1997; 99:S798–806.
79 Devillier P, Bousquet J. Inhibition of
the histamine-induced weal and flare
response: a valid surrogate measure
for antihistamine clinical efficacy?
Clin Exp Allergy 2007; 37:400–14.
80 Church MK, Maurer M. H(1)-antihista-
mines and urticaria: how can we pre-
dict the best drug for our patient?
Clin Exp Allergy 2012; 42:1423–9.
81 Bagenstose SE, Levin L, Bernstein JA.
The addition of zafirlukast to cetiri-
zine improves the treatment of
chronic urticaria in patients with
positive autologous serum skin test
results. J Allergy Clin Immunol 2004;
113:134–40.
82 Pacor ML, Di Lorenzo G, Corrocher R.
Efficacy of leukotriene receptor
antagonist in chronic urticaria. A
double-blind, placebo-controlled com-
parison of treatment with montelukast
and cetirizine in patients with chronic
urticaria with intolerance to food
additive and/or acetylsalicylic acid.
Clin Exp Allergy 2001; 31:1607–14.
83 Perez C, Sanchez-Borges M, Capriles
E. Pretreatment with montelukast
blocks NSAID-induced urticaria and
angioedema. J Allergy Clin Immunol
2001; 108:1060–1.
84 Nettis E, Pannofino A, Cavallo E, Fer-
rannini A, Tursi A. Efficacy of mont-
elukast, in combination with
loratadine, in the treatment of delayed
pressure urticaria. J Allergy Clin
Immunol 2003; 112:212–3.
85 Minciullo PL, Saija A, Bonanno D,
Ferlazzo E, Gangemi S. Montelukast-
induced generalized urticaria. Ann
Pharmacother 2004; 38:999–1001.
86 Maurer M, Rosen K, Hsieh HJ et al.
Omalizumab for the treatment of
chronic idiopathic or spontaneous
urticaria. N Engl J Med 2013;
368:924–35.
87 Grattan CE, O’Donnell BF, Francis DM
et al. Randomized double-blind study
of cyclosporin in chronic ‘idiopathic’
urticaria. Br J Dermatol 2000;
143:365–72.
88 Boubouka CD, Charissi C, Kouimintzis
D, Kalogeromitros D, Stavropoulos
PG, Katsarou A. Treatment of autoim-
mune urticaria with low-dose cyclo-
sporin A: a one-year follow-up. Acta
Derm Venereol 2011; 91:50–4.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 563

89 Shahar E, Bergman R, Guttman-Yas-
sky E, Pollack S. Treatment of severe
chronic idiopathic urticaria with oral
mycophenolate mofetil in patients not
responding to antihistamines and/or
corticosteroids. Int J Dermatol 2006;
45:1224–7.
90 Fedorowicz Z, van Zuuren EJ, Hu N.
Histamine H2-receptor antagonists for
urticaria. Cochrane Database Syst Rev
2012; 3:CD008596.
91 Simons FE, Sussman GL, Simons KJ.
Effect of the H2-antagonist cimetidine
on the pharmacokinetics and pharma-
codynamics of the H1-antagonists
hydroxyzine and cetirizine in patients
with chronic urticaria. J Allergy Clin
Immunol 1995; 95:685–93.
92 Paul E, Bodeker RH. Treatment of
chronic urticaria with terfenadine and
ranitidine. A randomized double-blind
study in 45 patients. Eur J Clin Phar-
macol 1986; 31:277–80.
93 Cicardi M, Banerji A, Bracho F et al.
Icatibant, a new bradykinin-receptor
antagonist, in hereditary angioedema.
N Engl J Med 2010; 363:532–41.
94 Bowen T, Cicardi M, Farkas H et al.
2010 International consensus algorithm
for the diagnosis, therapy and manage-
ment of hereditary angioedema. Allergy
Asthma Clin Immunol 2010; 6:24.
95 Bas M, Greve J, Stelter K et al. Therapeu-
tic efficacy of icatibant in angioedema
induced by angiotensin-converting
enzyme inhibitors: a case series. Ann
Emerg Med 2010; 56:278–82.
96 Rajan JP, Simon RA, Bosso JV. Preva-
lence of sensitivity to food and drug
additives in patients with chronic idi-
opathic urticaria. J Allergy Clin
Immunol Pract 2014; 2:168–71.
97 Nettis E, Colanardi MC, Ferrannini A,
Tursi A. Suspected tartrazine-induced
acute urticaria/angioedema is only
rarely reproducible by oral rechallenge.
Clin Exp Allergy 2003; 33:1725–9.
98 Rorie A, Goldner WS, Lyden E, Poole
JA. Beneficial role for supplemental
vitamin D3 treatment in chronic urti-
caria: a randomized study. Ann Allergy
Asthma Immunol 2014; 112:376–82.
99 Leech S, Grattan C, Lloyd K et al. The
RCPCH care pathway for children
with urticaria, angio-oedema or mast-
ocytosis: an evidence and consensus
based national approach. Arch Dis
Child 2011; 96(Suppl. 2):i34–7.
100 Greaves MW. Chronic urticaria in
childhood. Allergy 2000; 55:309–20.
101 Levy Y, Segal N, Weintrob N, Danon
YL. Chronic urticaria: association
with thyroid autoimmunity. Arch Dis
Child 2003; 88:517–9.
102 Stiehm ER. Immunologic disorders in
infants and children. 4th edn. Phila-
delphia: W.B. Saunders, 1996.
103 Krause K, Grattan CE, Bindslev-Jen-
sen C et al. How not to miss autoin-
flammatory diseases masquerading as
urticaria. Allergy 2012; 67:1465–74.
104 Zauli D, Grassi A, Granito A et al. Prev-
alence of silent coeliac disease in atop-
ics. Dig Liver Dis 2000; 32:775–9.
105 Gabrielli M, Candelli M, Cremonini F
et al. Idiopathic chronic urticaria and
celiac disease. Dig Dis Sci 2005;
50:1702–4.
106 Caminiti L, Passalacqua G, Magazzu
G et al. Chronic urticaria and associ-
ated coeliac disease in children: a
case-control study. Pediatr Allergy
Immunol 2005; 16:428–32.
107 The diagnosis and management of urti-
caria: a practice parameter part I: acute
urticaria/angioedema part II: chronic
urticaria/angioedema. Joint Task Force
on Practice Parameters. Ann Allergy
Asthma Immunol 2000; 85:521–44.
108 Farkas H. Pediatric hereditary angioe-
dema due to C1-inhibitor deficiency.
Allergy Asthma Clin Immunol 2010;
6:18.
109 Du-Thanh A, Raison-Peyron N, Drou-
et C, Guillot B. Efficacy of tranexamic
acid in sporadic idiopathic bradykinin
angioedema. Allergy 2010; 65:793
–5.
110 Sussman G, Hebert J, Barron C et al.
Real-life experiences with oma-
lizumab for the treatment of chronic
urticaria. Ann Allergy Asthma Immu-
nol 2014; 112:170–4.
111 Kaplan A, Ledford D, Ashby M et al.
Omalizumab in patients with symp-
tomatic chronic idiopathic/spontane-
ous urticaria despite standard
combination therapy. J Allergy Clin
Immunol 2013; 132:101–9.
112 Aselton P, Jick H, Milunsky A, Hunter
JR, Stergachis A. First-trimester drug
use and congenital disorders. Obstet
Gynecol 1985; 65:451–5.
113 Jick H, Holmes LB, Hunter JR, Mad-
sen S, Stergachis A. First-trimester
drug use and congenital disorders.
JAMA 1981; 246:343–6.
114 Kallen B. Use of antihistamine drugs
in early pregnancy and delivery out-
come. J Matern Fetal Neonatal Med
2002; 11:146–52.
115 Diav-Citrin O, Shechtman S, Aharon-
ovich A et al. Pregnancy outcome
after gestational exposure to lorata-
dine or antihistamines: a prospective
controlled cohort study. J Allergy Clin
Immunol 2003; 111:1239–43.
116 Einarson A, Bailey B, Jung G, Spizzirri
D, Baillie M, Koren G. Prospective con-
trolled study of hydroxyzine and cetir-
izine in pregnancy. Ann Allergy
Asthma Immunol 1997; 78:183–6.
117 Heinonen OP, Slone D, Shapiro S.
Birth defects and drugs in pregnancy.
Littleton, MA: Publishing Sciences
Group, 1977.
118 Hilbert J, Radwanski E, Affrime MB,
Perentesis G, Symchowicz S, Zampa-
glione N. Excretion of loratadine in
human breast milk. J Clin Pharmacol
1988; 28:234–9.
119 Briggs GB, Freeman RK, Yaffe SJ.
Drugs in pregnancy and lactation. 6th
Edn. Philadelphia: Lippincott Wil-
liams & Wilkins, 2001.
120 Zuberbier T, Oanta A, Bogacka E et al.
Comparison of the efficacy and safety
of bilastine 20 mg vs levocetirizine 5
mg for the treatment of chronic idio-
pathic urticaria: a multi-centre, double-
blind, randomized, placebo-controlled
study.
Allergy 2010; 65:516–28.
121 O’Donnell BF, Barr RM, Black AK
et al. Intravenous immunoglobulin in
autoimmune chronic urticaria. Br J
Dermatol 1998; 138:101–6.
122 Di Lorenzo G, Pacor ML, Mansueto P
et al. Randomized placebo-controlled
trial comparing desloratadine and
montelukast in monotherapy and
desloratadine plus montelukast in
combined therapy for chronic idio-
pathic urticaria. J Allergy Clin Immu-
nol 2004; 114:619–25.
123 Finn AF Jr, Kaplan AP, Fretwell R, Qu
R, Long J. A double-blind, placebo-
controlled trial of fexofenadine HCl
in the treatment of chronic idiopathic
urticaria. J Allergy Clin Immunol
1999; 104:1071–8.
124 Hindmarch I, Johnson S, Meadows R,
Kirkpatrick T, Shamsi Z. The acute
and sub-chronic effects of levocetiri-
zine, cetirizine, loratadine, prometh-
azine and placebo on cognitive
function, psychomotor performance,
and weal and flare. Curr Med Res
Opin 2001; 17:241–55.
125 Monroe EW, Fox RW, Green AW et al.
Efficacy and safety of loratadine (10
mg once daily) in the management of
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
564 R. J. Powell et al

idiopathic chronic urticaria. JAm
Acad Dermatol 1988; 19:138–9.
126 Dubertret L, Murrieta AM, Tonet J.
Efficacy and safety of mizolastine 10
mg in a placebo-controlled compari-
son with loratadine in chronic idio-
pathic urticaria: results of the MILOR
Study. J Eur Acad Dermatol Venereol
1999; 12:16–24.
127 Mullol J, Bousquet J, Bachert C et al.
Rupatadine in allergic rhinitis and
chronic urticaria. Allergy 2008; 63
(Suppl. 87):5–28.
128 Reimers A, Pichler C, Helbling A,
Pichler WJ, Yawalkar N. Zafirlukast
has no beneficial effects in the treat-
ment of chronic urticaria. Clin Exp
Allergy 2002; 32:1763–8.
129 Cicardi M, Bergamaschini L, Zingale
LC, Gioffre D, Agostoni A. Idiopathic
nonhistaminergic angioedema. Am J
Med 1999; 106:650–4.
130 Laurberg G. Tranexamic acid (Cy-
klokapron) in chronic urticaria: a
double-blind study. Acta Derm Vene-
reol 1977; 57:369–70.
131 Zimmerman AB, Berger EM, Elmariah
SB, Soter NA. The use of mycopheno-
late mofetil for the treatment of autoim-
mune and chronic idiopathic urticaria:
experience in 19 patients. J Am Acad
Dermatol 2012; 66:767–70.
132 Kessel A, Bamberger E, Toubi E.
Tacrolimus in the treatment of severe
chronic idiopathic urticaria: an open-
label prospective study. J Am Acad
Dermatol 2005; 52:145–8.
133 Shekelle PG, Woolf SH, Eccles M,
Grimshaw J. Clinical guidelines:
developing guidelines. BMJ 1999;
318:593–6.
134 British guideline on the management
of asthma. Thorax 2003; 58(Suppl. 1):
i1–94.
135 Eiser AR, Singh P, Shanies HM. Sus-
tained dapsone-induced remission of
hypocomplementemic urticarial vas-
culitis
–a case report. Angiology 1997;
48:1019–22.
136 Gonzalez P, Soriano V, Caballero T,
Niveiro E. Idiopatic angioedema trea-
ted with dapsone. Allergol Immuno-
pathol (Madr) 2005; 33:54–6.
137 Engin B, Ozdemir M. Prospective ran-
domized non-blinded clinical trial on
the use of dapsone plus antihistamine
vs. antihistamine in patients with
chronic idiopathic urticaria. J Eur Acad
Dermatol Venereol 2008; 22:481–6.
138 Reeves GE, Boyle MJ, Bonfield J,
Dobson P, Loewenthal M. Impact of
hydroxychloroquine therapy on
chronic urticaria: chronic autoim-
mune urticaria study and evaluation.
Intern Med J 2004; 34:182–6.
139 Gach JE, Sabroe RA, Greaves MW, Black
AK. Methotrexate-responsive chronic
idiopathic urticaria: a report of two
cases. Br J Dermatol 2001; 145:340–3.
140 Stack PS. Methotrexate for urticarial
vasculitis. Ann Allergy 1994; 72:36–8.
141 Parsad D, Pandhi R, Juneja A. Stan-
ozolol in chronic urticaria: a double
blind, placebo controlled trial. J Der-
matol 2001; 28:299–302.
142 Engler RJ, Squire E, Benson P.
Chronic sulfasalazine therapy in the
treatment of delayed pressure urti-
caria and angioedema. Ann Allergy
Asthma Immunol 1995; 74:155–9.
143 Jaffer AM. Sulfasalazine in the treat-
ment of corticosteroid-dependent
chronic idiopathic urticaria. J Allergy
Clin Immunol 1991; 88:964–5.
144 McGirt LY, Vasagar K, Gober LM,
Saini SS, Beck LA. Successful treat-
ment of recalcitrant chronic idio-
pathic urticaria with sulfasalazine.
Arch Dermatol 2006; 142:1337–42.
145 Parslew R, Pryce D, Ashworth J,
Friedmann PS. Warfarin treatment of
chronic idiopathic urticaria and
angio-oedema. Clin Exp Allergy 2000;
30:1161–5.
146 Pollack CV Jr, Romano TJ. Outpatient
management of acute urticaria: the
role of prednisone. Ann Emerg Med
1995; 26:547–51.
147 Leurs R, Church MK, Taglialatela M.
H1-antihistamines: inverse agonism,
anti-inflammatory actions and car-
diac effects. Clin Exp Allergy 2002;
32:489–98.
148 British Thoracic Society, Scottish Inter-
collegiate Guidelines Network. British
guideline on the management of asthma.
Thorax 2003; 58(Suppl. 1):i1–94.
149 Sanada S, Tanaka T, Kameyoshi Y,
Hide M. The effectiveness of mont-
elukast for the treatment of anti-his-
tamine-resistant chronic urticaria.
Arch Dermatol Res 2005; 297:134–8.
150 White M, Rothrock S, Meeves S, Liao
Y, Georges G. Comparative effects of
fexofenadine and montelukast on
allergen-induced wheal and flare.
Allergy Asthma Proc 2005; 26:221–8.
151 Nettis E, Colanardi MC, Paradiso MT,
Ferrannini A. Desloratadine in combina-
tion with montelukast in the treatment
of chronic urticaria: a randomized, dou-
ble-blind, placebo-controlled study. Clin
Exp Allergy 2004; 34:1401–7.
152 Erbagci Z. The leukotriene receptor
antagonist montelukast in the treat-
ment of chronic idiopathic urticaria:
a single-blind, placebo-controlled,
crossover clinical study. J Allergy Clin
Immunol 2002; 110:484–8.
153 Nettis E, Dambra P, D’Oronzio L,
Loria MP, Ferrannini A, Tursi A.
Comparison of montelukast and fexo-
fenadine for chronic idiopathic urti-
caria. Arch Dermatol 2001; 137:99–
100.
154 Baskan EB, Tunali S, Turker T, Sari-
caoglu H. Comparison of short- and
long-term cyclosporine A therapy in
chronic idiopathic urticaria. J Derma-
tolog Treat 2004; 15:164–8.
155 Di Gioacchino M, Di Stefano F, Cav-
allucci E et al. Treatment of chronic
idiopathic urticaria and positive
autologous serum skin test with
cyclosporine: clinical and immuno-
logical evaluation. Allergy Asthma
Proc 2003; 24:285–90.
Supporting Information
Additional Supporting Information may be found in
the online version of this article:
Appendix A1. Patient information sheet - chronic
urticaria and angioedema in adults.
Appendix A2. Patient information sheet - chronic
urticaria and angioedema in children.
© 2015 John Wiley & Sons Ltd, Clinical & Experimental Allergy, 45 : 547–565
Urticaria and Angioedema BSACI guideline 565
