
1
UAMS TRANSITIONAL YEAR
RESIDENCY PROGRAM
2023- 2024

2
UNIVERSITY OF ARKANSAS FOR MEDICAL SCIENCES
COLLEGE OF MEDICINE
OFFICE OF
GRADUATE MEDICAL EDUCATION
TRANSITIONAL YEAR RESIDENCY PROGRAM
MANUAL
2023-2024
Jason Mizell, M.D.
Professor, Colorectal Surgery
Program Director, Transitional Year Residency
Please report corrections and changes to
Emma Johnson
Transitional Year, Program Coordinator
Telephone: (501) 526-1876
E-mail: EJohnson3@uams.edu
Website: https://medicine.uams.edu/transitionalyear/
Office of Academic Affairs: Graduate Medical Education
4301 W. Markham # 837
Little Rock, AR 72205

3
TABLE OF CONTENTS
INTRODUCTION
Philosophy and Purpose of a Transitional Year pg. 7
Program Sponsors and Duration pg 8
Program Leadership pg 8
Objectives and Criteria for Graduation pg 8
Faculty Roster pg 10
Resident Roster pg 11
EDUCATIONAL PROGRAM
Overall Goals & Objectives pg 13
Clinical Rotation Curriculum pg 15
Didactic Educational Curriculum pg 16
2022-2023 Didactic Schedule pg 17 - 19
Other Educational Curriculum pg 20-22
CLINICAL ROTATION GOALS & OBJECTIVES
Resident Responsibilities pg 27
Patient Logs pg 27
Procedure Logs pg 28
Clinical Rotation Descriptions/Goals & Objectives pg 27
RESIDENT POLICIES
Work Hours pg 30
Work Environment pg 33
Moonlighting pg 34
Supervision pg 35
Transitions of Care pg 39
Addressing Resident Concerns pg 40
Evaluation, Promotion, & Disciplinary Actions pg 41
Fatigue Management & Mitigation pg 45
Resident Well Being pg 48
Vacation, Sick, & Educational Leave pg 46
GENERAL INFORMATION
Emergency Resuscitation pg 55
Contractual Agreement pg 55

4
Holidays pg 55
Leave: Administrative/Professional/Educational
Library pg 55
Mailboxes pg 55
Name Badges pg 56
Pagers pg 55
Parking pg 56
Pay Schedules pg 56
Professional Liability Insurance pg 56
Tuition Discounts pg 56
Social Media pg 56
Resident Participation in Non-UAMS Activities/Public Service pg 57
Education Fund pg 57
Appendix
My Mistake Curriculum pg 59
My Reflection Curriculum pg 65
Case Based Presentation Forms pg 68
Vacation/Sick/Education Leave Form
Communication Contract
Work Hour Logging Instructions
Tri-Annual Review Form
Rotation Evaluation Forms
Didactic Evaluation Form
360 Multi Rater Evaluation Form
Final Summative Evaluation Form
Patient Log/Procedure Log
5
WELCOME!
Dear UAMS COM Transitional Year residents,
Congratulations on your recent completion of medical school and welcome to the UAMS College of
Medicine Transitional Year (TY) Residency Program! The last several months have been filled with major
transition and uncertainty, but I hope things will begin to settle down for you as you transition from
student to physician. You are now a part of a very noble and privileged profession. As you progress
through this sometimes challenging, but always educational, year, remember that your actions and
attitudes reflect on your colleagues, facility, and organization. Therefore, strive to keep your actions and
attitudes positive and in the best interest of your patients.
This handbook was designed to provide you with the necessary information to successfully complete the
Transitional Year Program. Program goals, requirements, evaluation methods, and responsibilities will
be outlined in this handbook. Prior to starting your internship, you will be expected to review the
Transitional Program Handbook and Institutional Guidelines. These references will answer most of your
questions about UAMS and the Transitional Year Program and set you on the right path to success.
Important concepts will also be reviewed and discussed with you during your orientation to the
program. You and your faculty will also receive an electronic copy of this handbook at the beginning of
each academic year.
As you make your transition to a house staff officer, there are many wonderful mentors and staff
physicians that will help you along the way. If you have questions throughout the year, you only need to
ask.
Again, congratulations and welcome. The Transitional Year team is here to assist in making your intern
year a positive and successful educational experience.
Most sincerely,
Jason S. Mizell MD FACS FASCRS
Professor of Surgery
Division of Colon and Rectal Surgery
Program Director, Transitional Year Residency
Director of Business of Medicine
UAMS College of Medicine
6
INTRODUCTION
“A great leader's courage to fulfill his vision comes
from passion, not position.”
~John C Maxwell

7
PROGRAM GOALS AND PHILOSOPHY
Traditionally, the Transitional Year is designed to fulfill the educational needs of medical school
graduates who:
1. Have chosen a career specialty for which the categorical program in graduate medical education
has, as a prerequisite, one year of fundamental clinical education (this education may also
contain certain specific experiences for development of desired skills).
2. Desire a broad-based year to assist them in making a career choice or specialty selection
decision.
3. Are planning to serve in public health organizations or on active duty in the military as general
medical officers or primary flight/undersea medicine physicians.
4. Desire or need to acquire at least one year of fundamental clinical education before entering
administrative medicine or non-clinical research.
However, issues have arisen regarding the increasing competitiveness for medical students to find a
residency position, thus leaving medical schools with unmatched graduating students. This is happening
nationwide and most critically and importantly in our very own state of Arkansas with our own medical
students. In a state with currently one allopathic medical school whose primary goal is to train
physicians to stay here and serve the citizens of our state, having students that graduate without a place
to train is problematic.
We want our own “unmatched” UAMS medical students to have an opportunity to continue their
training and do what they are passionate about---serving patients and families and providing for their
healthcare needs.
Therefore, a goal of the Transitional Year (TY) Residency Education Program of the University of
Arkansas for Medical Sciences (UAMS) is to provide a year of a broad based and well-balanced clinical
curriculum as a possible opportunity for unmatched individuals to continue their training in preparation
for a desired specialty, or an opportunity for those individuals who desire an additional year to assist
them in making a career choice or specialty selection decision.
This philosophical principle of the TY is implemented by the selection of students who have exhibited
professionalism and who remain enthusiastic about their primary identity as physicians. All aspects of
the educational program maintain the orientation that, as a physician, one accepts the responsibility
(with appropriate referral and consultation) of the diagnosis and treatment of patients.
Consistent with the overall goal and philosophical orientation of the program is the need to provide
specific educational experiences to residents who will have varying roles in the field of medicine.

8
Program Sponsors and Duration
The sponsoring institution for the Transitional Year program is the University of Arkansas for Medical
Sciences College of Medicine (UAMS COM), which is ultimately responsible for the Transitional Year
program and many other accredited residency and fellowship programs.
The designated sponsoring programs for the Transitional Year residency program are the Internal
Medicine and Emergency Medicine residencies at UAMS. Both of these residency programs are ACGME-
accredited programs and provide at least 25% of the required fundamental clinical skills training to
Transitional Year residents.
The duration of the UAMS COM Transitional Year program is one year.
Program Leadership
The Transitional Year program director (TY PD) has the authority and accountability for the operation of
the Transitional Year program. Your TY PD is Jason Mizell, MD. Dr. Mizell is a board-certified general
surgeon and colon and rectal surgeon. He completed his undergraduate degree at Louisiana Tech
University in Ruston, LA and his medical school training and residency training at Louisiana State
University Health Sciences Center in Shreveport, LA. He went on to complete his colorectal fellowship
training at Baylor University Medical Center in Dallas Texas. He has been a member of the College of
Medicine faculty since 2010.
Your program director is responsible for administering and maintaining an educational environment
conducive to educating the Transitional Year Resident in each of the Accreditation Council for Graduate
Medical Education (ACGME) competencies.
Dr. Mizell keeps an “open door” policy and is readily available to all Transitional Year residents.
Office: 501-686-6757
Cell: 501-551-9734
Email: jsmizell@uams.edu
Emma Johnson is the program coordinator for the Transitional Year Residency Program. She is
responsible for coordinating many of the important and required tasks for the program and residents.
Cell: 501-526-1876
Email: EJohnson3@uams.edu
Objectives and Criteria for Graduation
Criteria for graduation include successful completion of objectives set forth in all essential rotations in
the Transitional Year Residency Manual. Residents must successfully complete all residency
assignments for the prescribed 12 months of education as dictated by the Residency Review Committee
for the Transitional Year. Residents must satisfactorily demonstrate competency as defined by the
ACGME and measured by the residency. This includes any mechanism for measuring competencies,
such as rotation evaluation, 360° evaluations, milestones, and portfolios (including My Mistake
Curriculum, My Reflection Curriculum, and Case Presentation – see below for explanation) or any other
means that the residency uses for evaluation purposes.
The objective of the Transitional Year is to provide a well-balanced program of graduate medical
education in multiple clinical disciplines designed to facilitate the choice of and preparation for a specific
9
specialty. The Transitional Year will provide 13 4-week block rotations, which provide the educational
milieu that stimulates and fosters assimilation of the following basic medical competencies necessary to
function as an optimal health care provider:
1. Patient care that is evidence based, compassionate, and appropriate.
2. Medical knowledge of established and evolving clinical practices.
3. Practice based learning and improvement of quality of patient care
4. Interpersonal and communication skills that result in effective exchange of information with
patients, families, and other health care providers
5. Professionalism in the practice of medicine.
6. System based practice to provide optimal patient outcomes while being good stewards of
resources.

10
TRANSITIONAL YEAR RESIDENCY
FACULTY ROSTER
Program Director
Jason S Mizell, MD
Professor, Surgery
Sponsoring Program, Program Director
Keyur Vyas, MD
Associate Professor of Internal Medicine
Program Director, Internal Medicine
Sponsoring Program, Program Director
Sarah Greenberger, MD
Associate Professor of Emergency Medicine
Program Director, Emergency Medicine
Faculty
Michael Saccente, MD
Professor, Internal Medicine
Associate Program Director, Internal Medicine
Nhan Phan, MD
Assistant Professor, Emergency Medicine
Ben Guise, MD
Associate Professor, Psychiatry
Program Director, Psychiatry
Heather Moore, MD
Assistant Professor
Program Director, Hospice and Palliative Medicine
Kedar Jambhekar, MD MBBS
Associate Professor, Radiology
Mitchell Jenkins, MD
Assistant Professor, Internal Medicine, Infectious Disease
Fen Xia, MD, PhD. MS
Professor, Radiation Oncology
Program Director, Radiation Oncology
Rani Lindberg, MD
Assistant Professor, PM&R
Program Director, PM&R
Neil Masangkay, MD
Assistant Professor, Neurology
Program Director, Neurology
Katie Kimbrough, MD
Associate Professor, Surgery
Program Director, Surgery
Surgical Critical Care Fellowship
Riley Lide, MD
Assistant Professor of Anesthesiology
Program Director, Anesthesia
Abby Nolder, MD
Associate Professor, Otolaryngology
Program Director, Otolaryngology
Amy Phillips, MD
Associate Professor, OB/Gyn
Program Director, OB/Gyn
Molly Meek, MD
Associate Professor, Interventional Radiology
Program Director, Interventional Radiology
Shashank Kraleti, MD
Assistant Professor, Family Medicine
Program Director, UAMS
Marlon J Doucet, MD BCEM
Deputy Chief
Emergency Medicine Service Line
Central Arkansas VA Healthcare System

11
RESIDENT ROSTER
Address all residents' mail to Slot 837
Residency program telephone: (501) 526-1876
Grayson Glenn
501-628-8737
Lauren Gawey
405-694-0114
Priya Patel
630-615-1035
Micah Bowling
903-244-1571
12
EDUCATIONAL
PROGRAM
“Tell me and I forget. Teach me and I remember.
Involve me and I learn.”
~Benjamin Franklin

13
Transitional Year Residency: Overall Educational Goals and Objectives
The Transitional Year program curriculum is based on the 6 ACGME core competencies with a goal of
graduating PGY-1 residents who are considered “competent” (target level score of 4) in the defined
Transitional Year Milestones:
1. Patient Care: Residents must be able to provide patient care that is compassionate, appropriate,
and effective for the treatment of health problems and the promotion of health.
a. Residents will be able to obtain a comprehensive medical history.
b. Residents will be able to perform a comprehensive physical examination.
c. Residents will be able to integrate information to develop an appropriate differential
diagnosis.
d. Residents will be able to generate an appropriate diagnostic and therapeutic plan for
assigned patients.
e. Residents will be able to recognize urgent and emergent medical conditions and apply
basic principles of triage and resuscitation.
f. Residents will be able to apply basic preventative care, diagnosis, and treatment
guidelines, and educate patients about these guidelines.
g. Residents will demonstrate understanding of indications/contraindications and ability to
perform common basic procedures such as, but not limited to simple suturing,
laceration management, venipuncture, IV access, bladder catheter placement, arterial
puncture, and nasogastric tube placement.
2. Medical Knowledge: Residents must demonstrate knowledge of established and evolving
biomedical, clinical, epidemiological, and social-behavioral sciences, as well as the application of
this knowledge to patient care.
a. Residents will demonstrate knowledge of established and evolving biomedical, clinical,
epidemiological, and social-behavioral sciences and apply this knowledge to patient
care.
b. Residents will successfully pass appropriate licensing and certification examinations.
Ideally, residents will have completed and passed USMLE Step 3 by the end of the
Transitional Year Residency Program.
3. Practice-based Learning and Improvement: Residents must demonstrate the ability to
investigate and evaluate their care of patients, to appraise and assimilate scientific evidence and
to continuously improve patient care based on constant self-evaluation and life-long learning.
a. Residents will demonstrate self-directed assessment and learning by identifying
strengths, deficiencies, and limits in one’s knowledge and expertise and setting learning
and improvement goals.
b. Residents will locate, appraise, and assimilate evidence from valid sources by identifying
and performing appropriate learning activities and using information technology to
optimize learning.
c. Residents will implement or be involved in Quality Improvement project and/or
activities.
4. Interpersonal and Communication Skills: Residents must demonstrate interpersonal and
communication skills that result in the effective exchange of information and collaboration with
patients, their families and health professionals.
a. Residents will communicate effectively with patients, family, and the public as
appropriate across a broad range of socioeconomic and cultural backgrounds.
b. Residents will communicate effectively with physicians, other health professionals, and
health related agencies.

14
c. Residents will work effectively as a member or leader of a healthcare team or other
professional group.
d. Residents will maintain comprehensive, timely and legible medical records.
5. Professionalism: Residents must demonstrate a commitment to carrying out professional
responsibilities and an adherence to ethical principles.
a. Residents will display compassion, integrity, and respect for others as well as sensitivity
and responsiveness to diverse patient populations including (but not limited to) diversity
in gender, age, culture, race, religion, disabilities, and sexual orientation.
b. Residents will demonstrate knowledge about, respect for, and adherence to the ethical
principles relevant to the practice of medicine, remembering that responsiveness to
patients that supersedes self-interest in an essential aspect of medical practice.
c. Residents will have accountability to patients, society, and the profession.
d. Residents will take personal responsibility in maintaining emotional, physical, and
mental health.
6. Systems-based Practice: Residents must demonstrate an awareness of and responsiveness to
the larger context and system of health care, as well as the ability to effectively call on other
resources in the system to provide optimal health care.
a. Residents will coordinate patient care within various health care delivery settings.
b. Residents will work in interdisciplinary teams to enhance patient safety and improve
patient care quality.
c. Residents will practice and advocate for cost-effective, responsible care.

15
Transitional Year Clinical Rotation Curriculum
The Transitional Year Program consists of 13 4-week blocks of training. Five of these blocks are required
fundamental clinical skill (FCS) rotations. Two blocks are required selective months in fundamental
clinical skill areas. The remaining six blocks are elective rotations.
There are competency-based goals and objectives for each rotation you will do this academic year. You
must review these goals and objectives of that service prior to each rotation and discuss them with the
service faculty member during your orientation to the rotation. The current rotation goals and
objectives are available in this handbook as well as electronically on the Transitional Year Residency
Website. Additionally, the goals and objectives are sent to you via New Innovations.
Transitional Year Block Schedule Example
16
Didactic Educational Curriculum
Didactic Education Sessions
While on clinical rotation (required FCS, selective FCS, and electives), you are required to attend that
service’s/department’s didactic sessions. These include (but not limited to) such things as Grand
Rounds, Weekly Seminar, Morning Report, Journal Club, Case Conference, Morbidity and Mortality
Conference, and QI Conferences. Your attendance at these conferences will be monitored. You should
check with your upper level resident or faculty for the service at the beginning of each clinical rotation
for the didactic/conference schedule.
Transitional Year Didactic Education Sessions
As a group, you will be excused from clinical duties to meet with your PD each block rotation on the
dates noted below (all dates are for Tuesdays) from 12:00 pm to 5:00 PM. Each month will feature a
component of the year’s curriculum covering several clinical and professional development topics. In
addition, this is an opportunity to share your experiences, discuss issues that need to be addressed, and
fellowship with one another. These meetings are required unless you have been excused by program
leadership. Attendance is monitored.
Please remind your upper level resident at the beginning of each clinical rotation of your required
absence for the didactic sessions. Please have them contact Dr. Mizell or Emma Johnson should they
have questions or concerns.

17
Other Educational Curriculum Experiences
Quality Improvement/Patient Safety Educational Curriculum
Although you will receive QI/PS training on rotations throughout the year, we have three requirements
designed to give you the tools and experience to incorporate this practice throughout your career.
1) IHI Open School Training
Prior to completion of your Transitional Year Residency, you will have completed the IHI Open
School Modules. Completion certificates will be maintained in your training folder.
(http://www.ihi.org
)
2) My Mistake – A QI/PS Presentation
“My Mistake” is a tool designed to teach and evaluate the ACGME core competency of systems-
based practice (SBP). Making mistakes while practicing medicine will unfortunately always happen.
It is important for new physicians to understand that mistakes happen, admit their mistakes, realize
how mistakes occur, and use the lessons learned to try to ensure they and others do not repeat the
same mistake. Each intern will prepare a presentation outlining a mistake they made with an
analysis of this mistake. This will be formally presented to the group one time during designated
didactic meetings (similar to a department M&M conference).
My Mistake curriculum description and forms can be found in the appendix.
3) Case Presentation
TY residents are required to present in a case-based didactic session to other TY residents and
faculty. The TY resident will choose an interesting case encountered during a clinical rotation or a
medical question formulated from a patient encountered or discussed during a clinical rotation.
The TY program director is available to assist with mentoring for writing a case presentation. This
presentation will demonstrate that the TY resident is able to do such things as evaluate relevant
literature and decide if the literature supports the need to make a clinical change or manage a case
in a different manner. A didactic conference focusing on the “how to’s” of scholarly
activity/products, reviewing the literature, and accessing electronic medical literature will be
covered prior to the Case Presentations.
The initial proposal for the case-based discussion is due to the Program Director due by December 1,
2021. Case presentations will be performed on January 10
th
, 2023.
Case presentation forms can be found in the appendix.
Additional educational activities that are encouraged to help improve the educational experience during
the TY year are listed below:
1. Scholarly Activity
All UAMS COM TY trainees are required to participate in scholarly activity to graduate. Given the
length of the Transitional Year program, completion of the assignments outlined below have been
designed to meet the necessary minimum criteria.

18
a. Journal Club
TY residents actively participate in 5 TY specific Journal Clubs throughout the year. They are
required to present an analysis of a journal article of their choice and encouraged to choose
an article related to their specific area of interest. The resident presents 10 minutes of
background information, 10 minutes of discussion (includes interpretation of results, and
how conclusions affect our practice), and 10 minutes of questions/answers, including
statistics and study design. Please see didactic schedule for Journal Club dates.
b. Other Research
A TY resident may elect to participate in up to 1 month of an elective in research. The TY
resident will identify a research mentor and project. This must be approved by the TY
program director. Specific goals and objectives for the research month and project will be
outlined and presented to the TY program director.
2. Practice Based Learning and Improvement
My Reflection Portfolio Projects
UAMS COM TY Residents will complete a written assignment, reflecting upon a specific event or
learning point that was unique to a rotation or the healthcare system. This project does not need
references, only the resident’s thoughts about a situation they encountered and the lessons
learned. Examples include discussing an ethical dilemma that was faced and how it was handled,
summarizing a key medical lesson learned during the rotation, or discussing insight that was gained
about a specific aspect of the healthcare system during a clinical rotation. Residents submit their
written project to the TY program director. Feedback is given to the resident and the project is
evaluated using the evaluation form. The write up and the evaluation will be kept by the program
director in the TY resident’s file.
TY Residents will complete a total of two My Reflection Portfolio Projects, with one each due
December 1, 2022 and May 1, 2023. My Reflection description and forms can be found in the
appendix.
3. Professionalism
UAMS COM TY Residents will complete two online modules throughout the year at their own pace
but completing the module early in the year will be emphasized. The first module is from the
Institute for Healthcare Improvement (IHI). UAMS requires all incoming residents and fellows to
complete and earn the Institute on Healthcare Improvement (IHI) Basic Certificate in Quality and
Safety, within their first year of training. The goal is to fulfill the common program requirement that
ACGME has set for residents and fellows to be able to “…systematically analyze practice using
quality improvement (QI) methods and implement changes with the goal of practice improvement
and professionalism”, and to fulfill CLER Pathways requirements for resident education on patient
safety (PS Pathway 6) and quality improvement (Q Pathway 1). The link is:
https://my.ihi.org/Portal/rise/Contacts/ihi-create-account/create-account-complete.aspx
Additionally, TY Residents will complete the AAMC Medportal Professionalism: Self-Study Module.
The module serves as an introduction to the tenets of the ACGME’s Core Competency of
Professionalism. The link is:
https://www.mededportal.org/doi/10.15766/mep_2374-8265.250
19
4. Appreciative Inquiry
Appreciative Inquiry can be described as an approach which draws from positive psychology and
storytelling, to create an “alignment of strengths” that render weaknesses irrelevant (Druker in TEDx
Talks, 2014), hence empowering individuals and facilitate the resolution of given problems to enact
desired change. During each tri-annual review, the program director will verbally discuss and
review the resident’s appreciate inquiry regarding where they stand on their goals and future
plans.
Steps of the appreciative inquiry are below:
1. Define – What is my desired outcome?
2. Discovery – What are my strengths?
3. Dream – What would work well in the future to make this happen?
4. Design – What action do I need to take to make it happen?
5. Deploy – Taking the action.
20
Evaluation Methods
UAMS COM TY Residents are evaluated using multiple tools from multiple perspectives. Elements of
clinical competence will be assessed in writing frequently by direct faculty supervisors with subsequent
review by the Program Director. Evaluations by peer resident physicians, patients, nursing staff and
other paramedical personnel may be included at less frequent intervals.
Clinical Rotation Evaluations
For each clinical rotation, residents will be evaluated using a milestone-based evaluation in New
Innovations by at least one (and often more) supervising attending. This evaluation allows the attending
to evaluate the TY Resident on the six ACGME core competencies, utilizing the Milestones as
appropriate. An example of the evaluation form can be found in the appendix.
TY residents will have the opportunity to anonymously evaluate both faculty and the clinical rotation for
each clinical rotation. These evaluations will be completed in New Innovations.
360
o
Evaluations
360
o
evaluations are collected for each resident during the TY Resident’s Ambulatory Care experience.
An example of the 360
o
evaluation form can be found in the appendix.
Other Educational Curriculum Projects
For all assigned projects/examinations, including My Mistake, My Reflection and the semi-annual Clinical
Skills Center Standardized Patient, TY residents will receive written and/or verbal feedback of their
performance.
Tri-Annual Evaluations with Program Director
UAMS COM TY Residents will meet with the program director three times during the year to formally
review your evaluations, discuss your goals and accomplishments, and ensure that your medical
education is progressing well.
Transitional Year Program Clinical Competency Committee (TY CCC)
The TY CCC is an appointed committee that has the major responsibility for assisting the Program
Director in assuring a fair and equitable evaluation process for the Transitional Year Interns. This
freestanding committee meets at least quarterly. Members include: assistant program director(s),
sponsoring program directors, program directors or designees of disciplines regularly included in the
curriculum, and directors of medical education.
The TY CCC has the following responsibilities:
1. Review the ongoing academic and clinical performance of each intern to include rotation
evaluations, portfolio projects, OSCE performance, and other available evaluations.
2. Advise the program director regarding resident progress to include recommendations for
promotion/graduation as well as adverse actions, to include counseling, Program Level
Remediation (PLR), Academic Probation, or Termination.
3. Serve as a forum for interns to address an adverse action or evaluation.
4. Review, judge and assign appropriate Milestone level assessments at least twice yearly for
reporting to the ACGME.
21
A resident receiving any unsatisfactory evaluation during the year may be immediately reviewed by the
Program Director and any written recommendations made to him/her may include:
1. Specific corrective actions
2. Repeating a rotation
3. Academic warning status or probation
4. Suspension or dismissal, if prior corrective action, academic warning and/or probation has been
unsuccessful.
The resident may appeal an unsatisfactory evaluation by submitting a written request to appear before
the TY CCC in a meeting called by the Program Director. The TY CCC will review a summary of the
deficiencies of the resident, and the resident will have the opportunity to explain or refute the
unsatisfactory evaluation. After review, the decision of the TY CCC is final.
Final Summative Evaluation
At the completion of the residency program, the Program Director will prepare a final evaluation of the
clinical competence of the UAMS COM TY Resident. This evaluation will stipulate the degree to which
the resident has mastered each component of clinical competence – patient care, medical knowledge,
practice-based learning and improvement, interpersonal and communication skills, professionalism, and
systems-based practice. It will also include any special accommodations the resident may have had
which could affect or limit the resident’s scope of practice. In this evaluation, the Program Director will
verify that the UAMS COM TY resident graduates training in good academic standing and at the time of
the final summative evaluation is able to function at the level commensurate with completing one year
of post-graduate training. A copy of this summative evaluation template can be found in the appendix.
Program Evaluation
UAMS COM TY Residents are asked to complete anonymous year-end program evaluations that are
utilized to improve upon the program. Trainees are encouraged to bring feedback to the TY program
leadership. The annual program review is held in June each year. This is an opportunity for faculty,
staff, and residents to review the Transitional Year Program curriculum, requirements and feedback
from staff, interns, graduates, and supervisors. Steps are taken to make positive improvements in the
program annually based upon such evaluations.
Transitional Year Program Evaluation Committee (TY PEC)
The TY PEC is an appointed committee that has the major responsibility for conducting and monitoring
the activities of the Transitional Year Program. This freestanding committee meets at least quarterly.
Members of this committee include: the Transitional Year program director, assistant program
director(s), sponsoring program directors, program directors or designees of disciplines regularly
included in the curriculum, directors of medical education and a peer selected intern.
The TY PEC has the following responsibilities:
1. Plan, develop, implement, and evaluate education activities of the program.
2. Review and make recommendations for revision of competency-based curriculum goals and
objectives.
3. Address areas of non-compliance with ACGME standards.
22
4. Review the program annually using evaluations of faculty, residents, and others to ensure there
are adequate resources for the didactic and clinical curriculum prescribed; to ensure that interns
are educated in high-quality medical care based on scientific knowledge, evidence-based
medicine, and sound teaching by qualified educators; and to ensure educational opportunities
are equivalent to those provided first-year Interns who are within the categorical programs in
which Transitional Year Interns participate.
5. Maintain a record of those in attendance and actions taken.
6. Review ACGME letters of accreditation for sponsoring programs and to monitor areas of
noncompliance.
7. Monitor and track resident performance, faculty development, graduate performance, and
program quality at least annually.
23
Clinical Rotation
Goals & Objectives
“A good physician treats the disease, the great
physician treats the patient who has the disease”
~Dr. William Osler

24
All program requirements for Transitional Year Residency training can be found at
http://www.acgme.org/Specialties/Program-Requirements-and-FAQs-and-
Applications/pfcatid/36/Transitional%20Year
UAMS Transitional Year Residency Program Resident Responsibilities
Responsibilities and competencies to be demonstrated in the first year of training:
1. Residents will perform accurate histories and physicals of hospitalized and ambulatory patients
in various settings. Residents will compile data, identify problems, prioritize problems, and
develop a differential diagnosis. These tasks will be performed under the supervision of more
senior residents and teaching faculty.
2. While rotating in the Emergency Department, residents will assess patients and perform focused
histories and physicals on patients under the supervision of an Emergency Medicine Attending.
3. Residents will enter admitting orders and daily orders for care under the supervision of more
senior residents and the attending faculty. Residents may enter orders in the ED, on the various
nursing units, and within the ICU’s.
4. Residents will respond to pages or calls from nursing units about assigned or cross-cover patient
problems. Residents will assess the problem and will seek advice from more senior residents or
from attending staff if the problem is beyond the experience and competency of the resident.
5. Residents will document the care provided and the assessments of the treating team in the
electronic medical record. Resident documentation will be reviewed by attending staff and
upper level residents; he or she will make the appropriate additions and or amendments to the
medical record.
6. Residents may have the opportunity to perform procedures under the supervision of either an
attending or in some cases an upper level resident or fellow. These procedures may include, but
are not limited to the following:
• Lumbar punctures
• Paracentesis
• Central line placement by the subclavian, femoral, or internal jugular approach
• Thoracentesis
• Arthrocentesis
• Bone marrow aspirates and biopsies
• Arterial puncture and line placement
• Venous puncture and line placement
• NG tube placement
• Urinary bladder catheterization
7. Resident will be BLS and ACLS certified.
8. Residents will verbally present cases to faculty attending physicians in accordance with the
accepted format. Presentations will be used to facilitate the supervision of patient care and
assess the knowledge and clinical skills of the resident.
25
Resident Patient/Procedural Logs
The Accreditation Council for Graduate Medical Education (ACGME) requires a record maintained of
specific cases treated by residents in a manner which does not identify patients, but which illustrates
each resident's clinical experience in the program. This record must demonstrate that each resident has
met the educational requirements of the program with regard to variety of patients, diagnoses, and
treatment modalities. This record will be reviewed periodically with the program director or a designee,
and be made available to the ACGME Site Visitor of the program. Patient/Procedural logs will be turned
into the Program Coordinator at the end of each clinical rotation.
Documentation of Procedures
While on inpatient units, the opportunity will arise for residents to perform procedures upon their
assigned patients. Many hospitals and educational institutions require documentation of procedures
performed during training to grant the privilege to perform or teach these procedures. This includes
surgical/operative procedures as well as bedside procedures such as lumbar punctures, CVL placement,
NG tube placement, abdominal paracentesis, etc.
A permanent record of each resident’s training is kept in the residency office. It is the responsibility of
each resident to document procedures he or she performs for inclusion in this file.
See the Appendix for an example/template of a patient log and procedural log. These logs are to be
turned in to the Residency Program Office twice a year (Dec 1 and Jun 1).
26
RESIDENT
POLICIES
“You are remembered for the rules you break.”
~Douglas MacArthur

27
Purpose:
In compliance with the UAMS College of Medicine Graduate Medical Education Committee policies on
clinical and educational work hours/work environment and moonlighting, and in considering that the care
of the patient and educational clinical duties are of the highest priority, the following guidelines apply:
Policy:
1. Work hours are limited to 80 hours per week, averaged over a four-week period, inclusive of all
in-house call activities.
2. Vacation or leave days will be taken out of the numerator and the denominator for calculating
work hours, call frequency, and days off, i.e. if a resident is on vacation for one week, the hours
for that rotation will be averaged over the remaining three weeks.
3. Residents are provided one day in seven free from all educational and clinical responsibilities,
averaged over a 4-week period, inclusive of call. One day is defined as one continuous 24-hour
period free from all clinical, educational, and administrative activities.
4. To ensure adequate time for rest and personal activities, a 10-hour time period is provided
between daily work periods and after in-house call.
5. The TY Program Director must ensure that residents are provided appropriate back-up support
when patient care responsibilities are especially difficult or prolonged.
6. Backup coverage is provided if patient care/clinical care needs exceed the TY resident's ability or
create resident fatigue sufficient to jeopardize patient care or resident welfare. Qualified faculty
physicians supervise all patient care and oversee the entire clinical care team. Faculty physicians
are always available in person, by telephone, or pager. In general, the chief resident or senior
level resident also oversee the lower level resident and/or intern.
Any faculty or chief resident/senior level resident who notices clinical care needs exceeding a
resident's ability or fatigue sufficient to negatively affect the performance of a resident will
directly relieve the resident of clinical work.
TY residents are also encouraged to notify their attending faculty or upper level resident if they
are concerned about clinical care needs exceeding their ability. The TY resident will be relieved
of those clinical duties or modifications will be made to provide the clinical case load appropriate
Policy
Transitional Year Residency
Subject
Work Hours
Policy Requirements:
ACGME Common Program Requirements:
ACGME Program Requirements for GME in Transitional Year:
Version History:
Date Developed: 6/2017
Last Review/Revision: 6/2018, 1/2019, 6/2021
Replaces:

28
to their ability. TY residents are provided sleeping rooms if fatigue is the factor impacting clinical
care needs exceeding the resident's ability.
Logging Work Hours
Residents are expected to log work hours continuously on a monthly basis in New Innovations. The
program coordinator will monitor, track, and report monthly work hour compliance to the program
director. Residents who are noncompliant in logging hours will be contacted directly and will meet with
the program director. Residents who have work hour violations will also be notified and will meet with
the program director. The program director will work with the supervisor of the rotational experience
where the work hour violation occurred to resolve the issue(s).
On-Call Activities
The goal of on-call activities is to provide residents with continuity of patient care experiences throughout
a 24-hour period.
In-house Call
1. Occurs no more frequently than every fourth night, averaged over a four-week period.
2. Does not exceed 24 consecutive hours of continuous on-site work. However, residents may
remain at work for up to six additional hours to participate in didactic activities, transfer care
of patients, conduct outpatient clinics, and maintain continuity care.
3. No new patients, defined as any patient to whom the resident has not previously provided
care, may be accepted after 24 hours of continuous work.
At-home Call (pager call)
1. TY residents will not participate in at-home (pager call).
The resident is expected to be work during normal working hours, Monday through Friday. Additional
work hours include on-call duties. Night, weekend, and holiday call schedules are formulated by the chief
residents and depend on the specific educational rotation. Residents must be available by telephone or
pager while on-call. Specific call schedules and responsibilities are delineated in the written
goals/objectives of each rotation, which are reviewed with the resident at the beginning of the rotation.
Falsification of work hour data or pressure to cause the falsification of such data is considered egregious
behavior for residents and can result in disciplinary action to include dismissal. Faculty members are
governed by University policies and procedures and should be aware of and adhere to GME work hour
regulations. Residents must notify the Program Director of requests or pressure to work in excess of
work hours authorized by this policy.
The Program Director must establish, distribute, and implement formal written policies and procedures
governing work hours and work environment for residents, which comply with institutional GME policy
and the Common and Specialty-specific Program Requirements.
The TY Program will be committed to and responsible for promoting patient safety and resident well-
being in a supportive educational environment. The learning objectives of the program must not be
compromised by excessive reliance on residents to fulfill non-physician service obligations.
29
The Sponsoring Institution provides health care delivery systems to minimize residents’/fellows’ work
that is extraneous to the program’s goals and objectives. The educational experience must not be
compromised by excessive reliance to fulfill non-physician service obligations.
The Sponsoring Institution ensures access to food while working at all participating sites, sleep/rest
facilities available for residents/fellows, and security and safety measures appropriate to the
participating site.
The Sponsoring Institution and programs must provide an environment in which residents/fellows have
the opportunity to raise concerns and provide feedback without intimidation or retaliation.
The Sponsoring Institution will oversee and document resident/fellow engagement in patient safety,
quality improvement, appropriate supervision, and mechanisms for reporting inadequate supervision.
The GMEC shall monitor compliance with this policy through:
a. Annual ACGME Survey of residents,
b. Special Review Process for underperforming programs
c. Requests for Work Hour Exceptions.
Work Hours Exceptions
An RRC may grant exceptions for up to 10% or a maximum of 88 hours to individual programs based on
a sound educational rationale. The GMEC must review and formally endorse the exemption prior to
submission to the RRC according to the following procedures:
The Program Director must submit a written request for an exemption to the GMEC Chair. The request
must clearly document the following:
a. Patient Safety: Information must be submitted that describes how the program and
institution will monitor, evaluate, and ensure patient safety with extended resident work hours.
b. Educational Rationale: The request must be based on a sound educational rationale which
should be described in relation to the program's stated goals and objectives for the assignments,
rotations, and level(s) of training for which the increase is requested. Blanket exceptions for the
entire educational program should be considered the exception, not the rule.
c. Moonlighting Policy: Specific information regarding the program's moonlighting policies for
the periods in question must be included.
d. Call Schedules: Specific information regarding the resident call schedules during the times
specified for the exception must be provided.
e. Faculty Monitoring: Evidence of faculty development activities regarding the effects of
resident fatigue and sleep deprivation must be appended.
The Program Director will present the request in person to the GMEC for discussion.
If approved by the GMEC, the Designated Institutional Official (DIO) or the GMEC Chair will provide a
documented written statement of institutional endorsement of the proposal.
The Program Director must submit the request to the RRC according to the ACGME’s RRC Procedures for
Granting Duty Hours Exceptions. The proposal to the RRC must include a copy of this policy (which
contains the institution's written procedures and criteria for endorsing requests for an exception to the
work hours limits) and the current accreditation status of the program and of the sponsoring institution.

30
Purpose:
The Transitional Year (TY) Residency Program and the UAMS College of Medicine jointly ensure the
availability of adequate resources for resident education, as outlined in the specific program requirements
of the ACGME.
Policy:
1. Meals: Food is available for residents 24 hours a day while working in all institutions.
2. Call Rooms: Adequate and appropriate call rooms that are safe, quiet, and private are provided
for all residents who take in-house call.
3. Ancillary Support: Adequate ancillary support for patient care is provided. Except in unusual
circumstances, providing ancillary support is not the resident responsibility except for specific
educational objectives or as necessary for patient care. This is defined as, but not limited to, the
following: drawing blood, obtaining EKGs, transporting patients, securing medical records,
securing test results, completing forms to order tests and studies, monitoring patients after
procedures.
4. Mail: Individual mailboxes are assigned which are located TY residency work room.
5. E-mail: E-mail accounts are issued by UAMS and must be checked daily.
Policy
Transitional Year Residency
Subject
Work Environment
Policy Requirements:
ACGME Common Program Requirements: VI.
ACGME Program Requirements for GME in Transitional Year: VI.
Version History:
Date Developed: 6/2017
Last Review/Revision: 6/2018, 1/2019, 6/2021
Replaces:

31
Purpose:
In compliance with the ACGME Common Program Requirements, VI.F.5.c
Moonlighting:
TY Residents are not eligible to participate in any moonlighting activities, internal or external.
Policy
Transitional Year Residency
Subject
Moonlighting
Policy Requirements:
ACGME Common Program Requirements: VI.F.5
ACGME Program Requirements for GME in Transitional Year: VI.F.5
Version History:
Date Developed: 6/2017
Last Review/Revision: 3/2019, 6/2021
Replaces:

32
Purpose:
The Transitional Year Residency Program will supervise residents:
• to ensure the provision of safe and effective patient care.
• to ensure that the educational needs of the residents are met.
• to allow for progressive responsibility appropriate to the residents’ level of education,
competence, and experience.
• according to specific supervision requirements in the Transitional Year Residency Program
requirements.
Policy:
All residents must perform clinical duties under proper supervision. Supervision will be defined by the
following classification:
• Direct Supervision: the supervising physician is physically present with the resident and the
patient.
• Indirect Supervision:
o With direct supervision immediately available – the supervising physician is physically
within the hospital or other site of patient care, and is immediately available to provide
direct supervision.
o With direct supervision available – the supervising physician is not physically present
within the hospital or other site of patient care but is immediately available by means of
telephonic and/or electronic modalities and is available to provide Direct Supervision.
• Oversight: the supervising physician is available to provide review of procedures/encounters
with feedback provided after care is delivered.
Procedure:
In compliance with the UAMS College of Medicine GME Committee policy on Resident Supervision, the
following guidelines are followed for supervision of TY residents:
Policy
Transitional Year Residency
Subject
Supervision of Residents
Policy Requirements:
ACGME Common Program Requirements: VI.A.2
ACGME Program Requirements for GME in Transitional Year: VI.A.2
Version History:
Date Developed: 6/2017
Last Review/Revision: 6/2018, 2/2019, 6/2021
Replaces:

33
1. Qualified faculty physicians supervise all patient care at each participating site and their
schedules are structured so that adequate supervision is available at all times.
2. Rapid, reliable systems for communication with supervisory physicians are available including
paging systems and cell phone access.
3. Attending faculty physician supervision is provided appropriate to the skill level of the residents
on the service/rotations.
4. Residents have progressive responsibility according to their level of education, competence, and
experience.
5. Specific responsibilities for patient care are included in the written description of each
service/rotation; this information is reviewed with the resident at the beginning of the
service/rotation. In general, the chief or senior level resident oversees the lower level resident
at the beginning of each service/rotation or if/when there is a change in the schedule. The
attending faculty oversees the entire team also providing direct and indirect supervision.
ACGME program requirements specify the following:
1. Each resident must know the limits of his/her scope of authority, and the circumstances under
which he/she is permitted to act with conditional independence.
2. In particular, PGY-1 residents are supervised either directly or indirectly with direct supervision
immediately available.
3. PGY-1 residents progress to being supervised indirectly with direct supervision available only
after demonstrating competence in:
o the ability and willingness to ask for help when indicated;
o gathering an appropriate history;
o the ability to perform an emergent assessment
o presenting patient findings and data accurately to a supervisor who has not seen the
patient.
Supervision and Responsibilities
Inpatient/Ward Services
TY residents (PGY 1-residents) in their first year of training are responsible for day-to-day management
of patients admitted to the inpatient services in which they are rotating. On admission, a complete
history and physical should be performed by the PGY-1 resident and charted in the permanent medical
record. Essentially, all admissions as well as daily orders are to be written by the resident, primarily the
intern and secondarily the upper level resident. Orders are not ordinarily written by the attending
physician or consultation services unless agreed upon by the residents. Specialized orders
(chemotherapy, dialysis, etc.) should be written by the subspecialty service. The PGY-1 resident is also
expected to see each patient at least twice daily and to write a daily progress note. Medical students
should be encouraged to write a history and physical and progress notes on each patient they follow;
however, these are in addition to the required PGY-1 resident notes. At the time of discharge, the PGY-1

34
resident is responsible for composing a written discharge note and completing discharge orders in a
timely manner. Whenever possible, these orders should be written the day prior to the patient’s
discharge.
Attending Physicians in Ward Services:
The attending physician is expected to see every patient within 24 hours of admission. He/she is to
write a note describing and confirming the patient’s history, examination, problem, and the diagnostic
and therapeutic plans. The attending physician is also encouraged to discuss topics relevant to the
patients on the service with the students, PGY-1, and upper level residents. The attending physician is
to see every patient on the service daily and to write a daily progress note. The attending must take
responsibility to ensure that all of the clinical decisions made on the patient are appropriate. Residents
are to be taught how to arrive at those decisions, and as competence is proven the resident should be
given the opportunity to make supervised clinical decisions. Orders should not be written by the
attending physician except in rare circumstances. He or she must be certain that therapy is appropriate,
that diagnostic studies and particularly invasive procedures are necessary, cost-effective and efficient,
and that high-quality care is provided.
The attending also has an obligation to provide high quality instruction in diagnosis, treatment, and
pathophysiology to both the residents and students on the service.
Intensive Care Units
The TY resident (PGY-1 resident) and the upper level resident (PGY-2, 3, or 4) are expected to interview
and examine every patient promptly on admission to the MICU or when called for a critical patient in
the emergency department or on a ward. After that is completed and any urgently needed investigation
or therapeutic measures have been discussed with the upper level resident and instituted, the fellow
and the attending physician on the service should be notified of the patient's admission and condition.
In critically ill patients, very frequent observations and examinations are required. The resident must be
aware of minute-to-minute changes in the patient’s condition. The upper level resident is expected to
make decisions and to be the primary caregiver for the patient by exercising keen clinical judgment and
seeking advice, support and agreement from the fellow and attending physician. As on the ward
services, the PGY-1 resident should be responsible for the writing of orders; however, as the patients are
critically ill there will be more instances when orders are written on an emergent basis by the upper
level resident, fellow, or attending. Orders are not to be written by consultation services except as
outlined above. The responsibility for the medical record is the same as on the ward service (see above).
It is expected that rotations in the intensive care units will provide experience in invasive procedures.
The upper level resident may undertake or supervise the PGY-1 resident on procedures with which he or
she has had adequate experience. Critical patients often require procedures (e.g. pulmonary artery
catheterization, elective cardioversion) that are done rarely out of an ICU setting. In these cases, the
procedure must be supervised by a fellow or attending physician.
Attending Physicians in Intensive Care Units:
The attending physician is responsible for all of the patient's care during the time in the ICU. The
attending should be notified immediately of the patient's admission and should see each patient within
a few hours. An attending note should be written shortly after admission on every patient, and daily
progress notes are required. As on the ward services, education and teaching rounds are an important
part of the attending physician's responsibility.

35
Consultative Services
The TY resident (PGY-1) is expected to see promptly all patients on whom subspecialty consultations (i.e.
IM subspecialties, Neurology, Psychiatry, PM&R) are requested. The chart should be reviewed to
determine pertinent past history and investigations. The patient should be interviewed and a physical
examination performed. The resident should assemble pertinent laboratory data, other diagnostic
studies, and organize a concise presentation of the problem to the attending physician on the
consultation service. It is the resident's further responsibility to ensure that recommendations are
transmitted accurately with a well-organized chart note. The note should detail the reasons for the
suggested studies or changes in management and not be a list of directives to the ward team or to the
residents on another service. Personal or telephone communication to the primary team will vastly
improve the response to the consultation and is common courtesy. Daily follow-up visits to determine
results of studies suggested or responses to therapeutic changes are also necessary, as are daily notes.
Attending Physicians in Consultative Services:
The attending physician must look upon a consultation as not only an encounter to advise the physician
or group responsible for the patient regarding the patient's diagnosis, additional studies that might be
needed, or changes in therapy, but also as an education exchange for the resident on his/her service and
the team requesting the consult. When possible, the attending physician should speak with the
residents on the team that initiated the consultation request and express an opinion and the reasons for
suggestions for study or changes in treatment. A thorough initial consultation note must be written.
The attending physician must see the patient as is appropriate with subsequent documentation by a
chart note.
Ambulatory Services
The TY resident (PGY-1) is expected to see promptly all assigned patients in the UAMS Family Medicine,
Gynecology, Pediatrics, or subspecialty medicine ambulatory clinic visits. The chart should be reviewed
to determine pertinent past history and investigations. The patient should be interviewed, and a
physical examination performed. The resident should assemble pertinent laboratory data, other
diagnostic studies, and organize a concise presentation of the problem to the attending physician on the
ambulatory service. It is the resident's further responsibility to ensure that recommendations are
transmitted accurately with a well-organized clinic note. The note should detail the reasons for the
suggested studies or changes in management. Personal or telephone communication to the referral
physician team will vastly improve the response to the clinic visit and is common courtesy. Follow-up
visits to determine results of studies suggested or responses to therapeutic changes are often necessary.
Attending Physicians in Ambulatory Clinics:
The attending physician must look upon the ambulatory clinic visit as not only an encounter to provide
primary or tertiary specialty care to a patient, but also as an education exchange for the resident on his
or her service. When possible, the attending physician should speak with the residents on the team that
initiated the ambulatory clinic request and express an opinion and the reasons for suggestions for study
or changes in treatment. A thorough initial clinic note must be written. The resident will initially see
each patient on his/her own, and then see the patient second time with the attending. As the residents
show progress, the attending may only see selected patients a second time, especially if these are follow
up patients. The attending will see ALL new patients. The attending must be in the exam room during all
office procedures including, but not limited to joint injection, punch biopsy, cryotherapy for skin lesions,
toenail and callus trimming. The attending physician must see the patient as is appropriate with
subsequent documentation by a clinic note.

36
Purpose
In compliance with the UAMS College of Medicine Graduate Medical Education Committee policies on
work hours/work environment and moonlighting and in considering that the care of the patient and
educational clinical duties is of the highest priority, the following guidelines apply:
Transitions of Care
1. The Sponsoring Institution must facilitate professional development for faculty and
residents/fellows regarding effective transitions of care, and ensure sites engage in standardized
transitions of care consistent with the setting and type of patient care.
2. Programs must design clinical assignments to minimize the number of transitions in patient care
and inform all members of the health care team of attending physicians and residents currently
responsible for each patient’s care.
3. See GME Policy 3.800
Policy
Transitional Year Residency
Subject
Transitions of Care
Policy Requirements:
ACGME Institutional Requirements: III.B.3
ACGME Common Program Requirements: VI.E, VI.E.3
UAMS GMEC Policy: 3.800
Version History:
Date Developed: 6/2017
Last Review/Revision: 3/2019, 6/2021
Replaces:

37
Purpose
In accordance with ACGME institutional, program and GMEC policies on addressing resident concerns.
At times various issues resulting from miscommunication, stress, or inappropriate behavior may arise. In
compliance with the UAMS COM GME Committee Policy 1.400 on Addressing Concerns in a Confidential
and Protected Manner, the TY resident should follow these guidelines to raise and resolve issues of
concern in a confidential manner:
1. A resident should discuss the concern with the supervising, senior level resident or attending
physician or the resident’s assigned faculty advisor.
2. If the above discussion does not resolve the concern, the resident should meet with the Program
Director or his/her designee.
3. If the issue cannot be resolved by the Program Director, the resident should contact a member of
the Resident Council or the Associate Dean for Graduate Medical Education. Members of the
Resident Council can meet with the resident and offer advice on how to resolve or handle the
problem and if further steps are necessary. Based on the discussion and advice at this meeting,
the resident may resolve the problem, and no further action is necessary.
4. For serious issues for which confidentiality is of the utmost importance, the resident may seek
assistance directly from the Program Director and/or the Associate Dean for GME.
5. A mechanism for reporting a lapse in professionalism on the part of a UAMS College of Medicine
Physician (a faculty member, i.e. program director or attending physician, or resident) is available
through the i-safe webpage at https://apps.uams.edu/i-safe/. This is a confidential reporting
system that is reviewed by the Dean’s Senior Advisory Committee.
6. At any time a resident’s problem cannot be resolved, the Office of Human Resources may be
consulted and serve as another system of assistance/support.
Every effort is made to protect TY residents of mistreatment from retaliation, fear, or intimidation if they
seek redress. Retaliation will not be tolerated. To help prevent retaliation, those who are accused of
mistreatment or whom the concern has been raised will be informed that retaliation is regarded as a form
of mistreatment. Accusations that retaliation/intimidation/fear has occurred will be handled in the same
manner as accusations concerning other forms of mistreatment. (See GMEC policy 1.500).
Policy
Transitional Year Residency
Subject
Addressing Resident and Faculty Concerns
Policy Requirements:
ACGME Institutional Requirements: IV.D, III.A
ACGME Common Program Requirements: II.A.4.h
UAMS GMEC Policy: 1.400
Version History:
Date Developed: 6/2017
Last Review/Revision: 3/2019, 6/2021
Replaces:

38
Purpose
In accordance with ACGME institutional, program and GMEC policies on resident evaluation, promotion,
and disciplinary actions.
Evaluations
During the residency period the following elements of clinical competence will be assessed in writing
(using New Innovations) in a timely manner during each rotation or similar educational assignment by
attending faculty, chief residents, peers, students, self, and multi-raters (patient/family, nurses, social
workers, etc.) with subsequent review by the TY program director. A TY resident will meet with the
program director three times/year (typically Oct, Jan, May) to review results of evaluations and other
performance measures
Clinical competence requirements:
1. Patient Care: Gather essential, accurate patient information; order appropriate tests; make
accurate diagnoses; perform competently; counsel patients and families; prescribe appropriate
medication and treatment.
2. Interpersonal and Communicative Skills: Document pertinent information clearly; write legibly;
listen actively; use effective nonverbal behaviors; work effectively as a member of a team.
3. Medical Knowledge: Know and apply basic sciences; demonstrate analytical approach to clinical
care.
4. Practice-Based Learning and Improvement: Stay current with medical literature and technology;
analyze your experiences to improve your practice; facilitate learning of students and others.
5. Professionalism: Demonstrate integrity, honesty, and empathy; respect patients’ autonomy and
diversity; be timely and respond promptly.
6. Systems-Based Practice: Demonstrate an awareness of and responsiveness to the larger context
and system of health care, as well as the ability to call effectively on other resources in the
system to provide optimal health care.
In addition, the following assessments will be conducted for each resident:
1. The TY program director will meet with each TY resident tri-annually with a summative
evaluation at the end of the year.
2. The TY program director will prepare a summative evaluation for each tri-annual meeting that
will be reviewed with the TY resident and signed by both the TY resident and PD.
The TY Clinical Competency Committee, which is made up of individuals active in GME and with
prominent roles in their respective disciplines, will review all resident evaluations semi-annually, will
assist in preparation of milestone reports to the ACGME, and will advise the TY program director
regarding progress, remediation, and dismissal.
Policy
Transitional Year Residency
Subject
Evaluation, Promotion, and Disciplinary Actions
Policy Requirements:
ACGME Institutional Requirements: IV.C
ACGME Program Requirements for GME in Transitional Year: V.
UAMS GMEC Policy: 1.300, 1.410, 1.420
Version History:
Date Developed: 6/2017
Last Review/Revision: 3/2019, 6/2021
Replaces:

39
The evaluations will be maintained in a confidential file and only available to authorized personnel.
Upon request, the TY resident my review his/her evaluation file at any time during the year. At the
completion of the Transitional Year Residency Program, the Program Director will prepare a final
summative evaluation of the clinical competence of the resident. This evaluation will stipulate the
degree to which the resident has mastered each component of clinical competence – patient care,
medical knowledge, practice-based learning and improvement, interpersonal and communication skills,
professionalism, and systems-based practice. It will also include any special accommodations the
resident may have had which could affect or limit the resident’s scope of practice. In this evaluation the
Program Director will verify that the resident “has demonstrated sufficient competence to enter
practice without direct supervision” and has “satisfactorily” completed the Transitional Year Residency
Program. This evaluation will remain in the resident’s permanent file to substantiate future judgments
in hospital credentialing, board certification, agency licensing, and in the actions of other bodies.
Probation/Suspension/Dismissal
Actions of probation/suspension/dismissal will follow the guidelines in the Graduate Medical Education
Committee Policy 1.440 on Academic Improvement and Disciplinary Actions Policy. In addition, specific
TY program guidelines follow:
1. A resident may be placed on probation by the Program Director for reasons including, but not
limited to any of the following:
a. failure to meet the performance standards of an individual rotation;
b. failure to meet the performance standards of the program;
c. failure to comply with the policies and procedures of the GME Committee, the UAMS
Medical Center, or the participating institutions
d. misconduct that infringes on the principles and guidelines set forth by the training
program;
e. documented and recurrent failure to complete medical records in a timely and
appropriate manner;
f. when reasonably documented professional misconduct or ethical charges are brought
against a resident which bear on his/her fitness to participate in the training program.
2. When a resident is placed on probation, the Program Director shall notify the resident in writing in
a timely manner, usually within a week of the notification of probation. The written statement of
probation will include a length of time in which the resident must correct the deficiency or
problem, the specific remedial steps, and the consequences of non-compliance with the
remediation.
3. Based upon a resident’s compliance with the remedial steps and other performance during
probation, a resident may be:
a. continued on probation;
b. removed from probation;
c. placed on suspension; or
d. dismissed from the residency program.
Suspension
1. A resident may be suspended from a residency program for reasons including, but not limited, to
any of the following:
a. failure to meet the requirements of probation;
b. failure to meet the performance standards of the program;

40
c. failure to comply with the policies and procedures of the GME Committee, the UAMS
Medical Center, or the participating institutions;
d. misconduct that infringes on the principles and guidelines set forth by the training
program;
e. documented and recurrent failure to complete medical records in a timely and
appropriate manner;
f. when reasonably documented professional misconduct or ethical charges are brought
against a resident which bear on his/her fitness to participate in the training program;
g. when reasonably documented legal charges have been brought against a resident which
bear on his/her fitness to participate in the training program;
h. if a resident is deemed an immediate danger to patients, himself or herself or to others;
i. if a resident fails to comply with the medical licensure laws of the State of Arkansas.
2. When a resident is suspended, the Program Director shall notify the resident with a written
statement of suspension to include:
a. reasons for the action;
b. appropriate measures to assure satisfactory resolution of the problem(s);
c. activities of the program in which the resident may and may not participate;
d. the date the suspension becomes effective;
e. consequences of non-compliance with the terms of the suspension;
f. whether or not the resident is required to spend additional time in training to
compensate for the period of suspension and be eligible for certification for a full
training year.
A copy of the statement of suspension shall be forwarded to the Associate Dean for Graduate Medical
Education and the Director of Housestaff Records.
3. During the suspension, the resident will be placed on “administrative leave,” with or without pay as
appropriate depending on the circumstances.
4. At any time during or after the suspension, the resident may be:
a. reinstated with no qualifications;
b. reinstated on probation;
c. continued on suspension; or
d. dismissed from the program.
Dismissal
Dismissal from a residency program may occur for reasons including, but not limited to, any of the
following:
a. failure to meet the performance standards of the program;
b. failure to comply with the policies and procedures of the GME Committee, the UAMS
Medical Center, or the participating institutions;
c. illegal conduct;
d. unethical conduct;
e. performance and behavior which compromise the welfare of patients, self, or others;
f. failure to comply with the medical licensure laws of the State of Arkansas;
g. inability of the resident to pass the requisite examinations for licensure to practice
medicine in the United States, if required by the individual residency program.
2. The Program Director shall contact the Associate Dean for GME and provide written documentation
which led to the proposed action.

41
3. When performance or conduct is considered sufficiently unsatisfactory that dismissal is being
considered, the Program Director shall notify the resident with a written statement to include:
a. reasons for the proposed action,
b. the appropriate measures and timeframe for satisfactory resolution of the problem(s).
4. If the situation is not improved within the timeframe, the resident will be dismissed.
5. Immediate dismissal can occur at any time without prior notification in instances of gross
misconduct including, but not limited to theft of money or property; physical violence directed at an
employee, visitor, or patient; use of or being under the influence of alcohol or controlled
substances while working; patient endangerment; or illegal conduct.
6. When a resident is dismissed, the Program Director shall provide the resident with a written letter of
dismissal stating the reason for the action and the date the dismissal becomes effective. A copy of
this letter shall be forwarded to the Associate Dean for GME and the Director of Housestaff Records.
A TY resident involved in the disciplinary actions of probation, suspension, and dismissal has the right to
appeal according to the Graduate Medical Education Committee Policy 1.410, Adjudication of
Resident/Fellow Grievances.
The TY resident may appeal an unsatisfactory evaluation by submitting a written request to appear
before the department’s Competency/Promotions Subcommittee of the Residency Education
Committee in a meeting called by the Program Director. The Committee will review a summary of the
deficiencies of the resident, and the resident will have the opportunity to explain or refute the
unsatisfactory evaluation. After review, the decision of this Committee is final.

42
Purpose:
In compliance with the UAMS College of Medicine Graduate Medical Education Committee policies on
work hours/work environment and moonlighting and in considering that the care of the patient and
educational clinical duties is of the highest priority, the following guidelines apply:
Policy:
1. Programs will educate faculty and residents in fatigue mitigation processes, in recognition of the signs
of fatigue and sleep deprivation, and have a fatigue mitigation plan such as napping, adjusting
schedules, or back up support including a process to ensure continuity of patient care should a faculty
member or resident be unable to perform his/her duties.
2. The program director will monitor individually as well as aggregate program use of the fatigue
mitigation process.
a. Individual monitoring for signs of fatigue should be at a minimum during the semi-annual
evaluation.
b. The program aggregate use of the fatigue mitigation process may indicate the need for
program wide changes.
3. The Sponsoring Institution provides nap facilities for residents who may be too fatigued to safely
return home.
4. Resources on the UAMS COM GME webpage include a 10-minute video on managing fatigue. In
addition, residents are required to participate in an interactive presentation which covers sleepiness and
fatigue given at orientation.
Policy
Transitional Year Residency
Subject
Fatigue Management and Mitigation
Policy Requirements:
ACGME Common Program Requirements: VI.D
ACGME Program Requirements for GME in Transitional Year: VI.D
Version History:
Date Developed: 6/2017
Last Review/Revision: 6/2018, 1/2019, 6/2021
Replaces:

43
Vacation
Residents receive 21 days (15 workdays plus weekend days) of paid vacation each year. This cannot be
"carried over" from one year to the next.
Residents may take no more than 1 week (7 days) of vacation leave at one time.
In addition to the annual vacation days that are given on a yearly basis, each resident will also be allotted
five (5) additional vacation days for use by the resident at their discretion during the entirety of the
individual’s residency period at UAMS.
Residents must submit vacation requests through New Innovations. Additionally, they must
notify the service they will be on of their vacation and make provisions when needed or
instructed. Vacation requests are encouraged to be submitted as early as possible to allow
for coverage, planning, and scheduling by the respective service.
Professional or Educational Leave
Residents receive a maximum of 5 days per year of professional educational leave. This is in addition to
sick and vacation time. Professional and educational leave may not be carried over from one year to the
next.
Job or further educational training interview days may not be counted as professional or educational
leave.
Professional or educational leave may be used to take primary or subspecialty boards.
USMLE exams may be taken using professional or educational leave.
For audit purposes, professional or educational leave must be noted as such on the schedule submitted
to the Housestaff Office.
Residents must submit professional or educational leave requests through New Innovations.
Additionally, they must notify the service they will be on of their planned leave and make
provisions when needed or instructed. Leave requests are encouraged to be submitted as
early as possible to allow for coverage, planning, and scheduling by the respective service.
Sick Leave
Policy
Transitional Year Residency
Subject
Vacation, Sick, Professional, or Educational Leave
Policy Requirements:
ACGME Institutional Requirements: II.D.4.h
UAMS GMEC Policy: 2.200
Version History:
Date Developed: 6/2017
Last Review/Revision: 3/2019, 6/2021
Replaces:

44
If a resident cannot come to work due to illness, they will notify the attending physician and/or upper
level resident of your current clinical rotation. Additionally, the resident will notify the TY program
coordinator and/or program director. If you have a planned medical leave or appointment, a
standard leave form should be submitted prior to the leave for planning purposes. Sick leave may not
be used for supplemental clinical activities, to interview for jobs or categorical residency positions, or
to relocate.
Residents have 12 days of sick leave (including weekend days if scheduled to work) for medical
reasons during each year of training. The sick leave cannot be “carried over” between years. Sick
leave in excess of 12 days requires special review by the Associate Dean and Program Director.
Residents must complete the vacation and educational leave request form found at the following link on
the TY website https://transitionalyear.uams.edu/current-residents/vacation-request-form/
.

45
Purpose
In accordance with Accreditation Council for Graduate Medical Education (ACGME) institutional and
program policies on addressing resident concerns.
In the current health care environment, residents and faculty members are at increased risk for burnout
and depression. Psychological, emotional, and physical well-being are critical in the development of the
competent, caring, and resilient physician. Self-care is an important component of professionalism; it is
also a skill that must be learned and nurtured in the context of other aspects of residency training.
Programs, in partnership with their Sponsoring Institutions, have the same responsibility to address
well-being as they do to evaluate other aspects of resident competence.
Policy
The Transitional Year (TY) is stressful for several reasons. First, like any first year intern, TY Residents are
suddenly given more responsibility than ever before. In addition, a TY Resident typically rotates to a
new department every month. Just as the TY Resident is starting to learn the system and feel
comfortable, it’s time to move on and the learning curve becomes steep once more. During the latter
half of the year, the TY Resident may be rotating on surgery or pediatrics or medicine for the first time
and the categorical residents will have already done this rotation multiple times. Remember – a TY
Residents is NEVER alone. There will always be an upper level resident or staff to help the TY Resident
make decisions and take care of patients. The other services greatly appreciate the TY Residents
rotating on their services.
To make the transition easier each month, the following should be remembered:
1. Get a good orientation to the rotation.
2. Don’t be afraid to ask questions. It is much better to ask a question than to do
something wrong. Don’t expect to know everything that the categorical residents know.
3. Get to know fellow TY Residents and their families. Do things as a group outside the
hospital.
4. Be good to yourself, your families, and your friends. Stay fit - do things that help you
relieve stress whether sleeping, running, playing sports, taking some time to be with
your spouse and kids and friends.
5. Residents with families need to make them a priority – remember you are blessed to
have them here with you for support.
6. Single residents also need to find time for friends and family that may live further away.
Stay engaged. Don’t let yourself become lonely.
Policy
Transitional Year Residency
Subject
Resident Well Being
Policy Requirements:
ACGME Institutional Requirements: III.B.7
ACGME Common Program Requirements: VI.C
Version History:
Date Developed: 6/2017
Last Review/Revision: 5/2019, 6/2021
Replaces:

46
The Transitional Year work room is available as a place to relax, spend time with other residents, get
work done, eat, and rest. Transitional Year residents, the Program Coordinator, and Program Director
are the only people who have access to the room, so the room can easily be utilized to “get away” when
needed.
Burnout Education
Why is it important to recognize burnout?
Unrecognized and/or untreated burnout can negatively impact many aspects of your life:
• Your work performance and patient safety.
• Your personal life.
• Your academic achievements.
Consequences of burnout may include but are not limited to the following:
• Feelings of dissatisfaction and non-enjoyment of life.
• Anxiety and depression and their consequences.
What to do to help burnout?
The following maybe helpful guidelines for assisting you in the way of improvement from burnout:
• Slow Down: cut back/decrease whatever commitments and activities that you can
• Get Support: turn to loved ones for support
• Re-evaluate: your goals and priorities
• Prioritize sleep: sleep improves mood and reduces burnout
Professional Help
In addition to any of a TY Resident’s other healthcare needs already in place, the following are other
options for professional help should a TY Resident experience burnout/depression or have other mental
health care needs.
Employee Assistance Program (EAP)
The Employee Assistance Program (EAP) consultation service provides assessment, short-term counseling,
information and referral (if indicated) for employees (including their spouses and dependents) who
experience some form of personal distress. Services are confidential and include but are not limited to
the following:
• Short-term, individual and family counseling
• Individual life skills training
• Life/career coaching
• Wellness training
• Grief/bereavement
• Personal/emotional concerns
• Anger management
• Stress management
Contact Information:
5800 W 10
th
Street, Suite 601
Little Rock, AR 72204
Voice: 501.686.2588
Toll Free: 1.800.542.6021

47
http://eap.uams.edu/services/employee-services/
House Staff Wellness Program
The following services are provided:
• Counseling/psychotherapy
• Medication treatment
Contact Information:
To schedule an appointment, or for further information call 501-686-8408 or email
residentwellness@uams.edu.
Please identify yourself as a College of Medicine House Staff member.
https://residentwellness.uams.edu/
Finally, your TY program director is available 24 hours a day, seven days a week in person, by phone or
pager to answer questions, help resolve conflicts and support you. Remember, your TY program
director has an open door policy. If you need assistance at any time, please stop by, call or email.
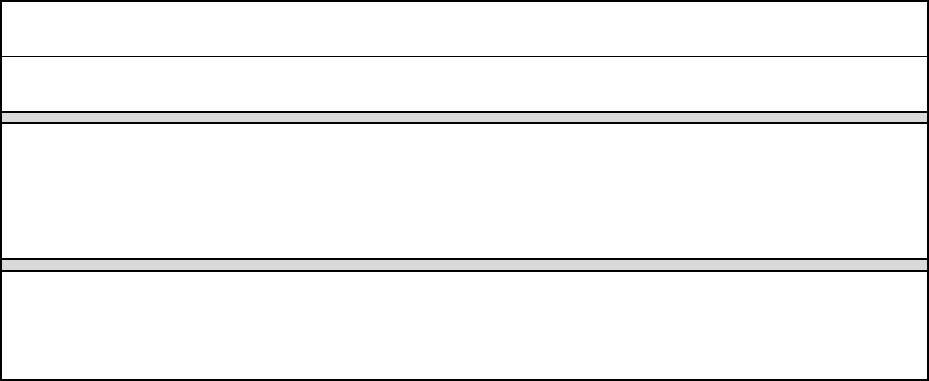
48
Policy
Transitional Year Residency
Subject
Recruitment and Appointment
Policy Requirements
ACGME Institutional: IV.A. & B
ACGME Common: I.C.; III.A.
UAMS Administrative Policy: 4.5.31, UAMS Medical Center Policy HR. 3.02.
UAMS GMEC Policy : 1.200
Version History
Date developed: 8/2019
Replaces:
Revisions Approved: 11/2020
Purpose
To define the requirements and procedures for the recruitment and appointment of residents to
Accreditation Council for Graduate Medical Education (ACGME) accredited Transitional Year Programs
sponsored by the University of Arkansas for Medical Sciences College of Medicine (UAMS COM). To
define the process for monitoring this program for compliance.
Policy
A. The recruitment and appointment of residents to programs sponsored by the UAMS COM is based
on and is in compliance with the institutional, common, and specific program requirements of the
ACGME.
B. In accordance with the UAMS Graduate Medical Education Committee Policy 1.200, each
program must establish and implement written policies and procedures for the eligibility,
application, and selection processes of residents based on this policy. Each program’s written
procedure will include the criteria, including requirements related to a resident ability to
perform clinical and other duties, and procedure used by the program to select residents and
the length of time the program keeps the applications on file. Implementation of the program
policy is the responsibility of the Departmental Chairperson, the Program Director, and/or
departmental faculty.
C. National Resident Matching Program (NRMP) Match Participation Agreement for Application and
Programs (5.1 Match Commitment) states that failure to start the training program on the date
specified in the appointment contract, without a waiver from the NRMP, constitutes a breach of
the Match Agreement and may result in penalties.
E. This program must not discriminate with regard to sex, race, age, religion, color, national origin,
disability, veteran status, or genetics. The program must have policies and procedures related to
recruitment and retention of a diverse and inclusive workforce.
F. This program’s compliance with the terms of this policy is monitored annually when the
Program Director and/or Program Coordinator submits to the Director of Housestaff Records
verification that all incoming residents of the program meet the eligibility requirements.
49
G. Transfers must meet eligibility and selection criteria and successfully complete the criminal
background check. Program must ensure that Graduate Medical Education (GMEC) policy 1.210
on Resident Transfers has been followed.
H. Health insurance benefits will begin for the residents and their family on the first officially
recognized day of the program.
I. If an applicant’s required training time will extend beyond the initial residency period (IRP)
assigned by Centers for Medicare and Medicaid Services (CMS) for funding, programs must
verify that additional funds are available through the appropriate GME mechanism. An example
is a resident who changes programs by re-entering the Match, since CMS does not ever assign a
new IRP.
J. All candidates for residency programs are subject to background checks subject to UAMS
Administrative policy 4.5.31 and UAMS Medical Center policy HR. 3.02.
Procedure
Recruitment
An applicant must meet one of the following qualifications to be eligible for appointment to an
ACGME-accredited program:
a) graduation from a medical school in the United States or Canada, accredited by the
Liaison Committee on Medical Education (LCME); or,
b) graduation from a college of osteopathic medicine in the United States, accredited
by the American Osteopathic Association (AOA); or,
c) graduation from a medical school outside of the United States or Canada,
and meeting one of the following additional qualifications: holds a currently-valid
certificate from the Educational Commission for Foreign Medical Graduates prior to
appointment; or, holds a full and unrestricted license to practice medicine in a
United States licensing jurisdiction in his or her current ACGME
specialty/subspecialty program; or, has graduated from a medical school outside the
United States and has completed a Fifth Pathway** program provided by an LCME-
accredited medical school.
In addition to ACGME requirements, the following apply:
a) Since pursuing a career in Arkansas is desired, no program shall admit a
resident/fellow that the Arkansas State Medical Board (ASMB) will not consider for
an Arkansas license. See Arkansas Medical Practices Act 17-95-401 through 17-95-
407 on Licensing, Regulations 3 & 14 of the Regulations of the Arkansas State
Medical Board.
b) Successful completion of any step of the USMLE or COMLEX in no more than 3
attempts per step (ASMB Regulations 3 & 14).
c) An applicant must demonstrate the following English language proficiency:
1. Proficiency in reading and writing (printing) English text;
2. Proficiency in understanding spoken English on conversational and
medical topics;
3. Proficiency in speaking English on conversational and medical topics.
50
Any appointed resident found to be in violation of the English proficiency eligibility
requirement will be referred, at the expense of the program, for appropriate
remediation.
d) The ability to reside continuously in the U.S. for the entire length of training.
Appointment
The Resident Agreement of Appointment is for the duration of no longer than 1 year.
A resident is considered appointed in the COM when all required onboarding processes have been
successfully completed.
51
GENERAL
INFORMATION
“Success is not final, failure is not fatal: it is the
courage to continue that counts.”
~Winston Churchill

52
Emergency Resuscitation
Emergency resuscitation is provided anywhere on the UAMS campus including hospital wards
by an emergency code team. The team may be summoned by dialing 686-7333 and having the
hospital operator announces a code. Check the victim's respiration and pulse and provide Basic Life
Support until team arrives. Advanced Cardiac Life Support (ACLS) protocols are followed by
the team, and all team members must be certified ACLS Providers to participate. If you are on an
Internal Medicine rotation, you must complete an ACLS Provider Course before taking this call.
Contractual Agreement
House staff appointments are for a period not exceeding one year. A house staff agreement
outlining the general mutual responsibility of the College of Medicine and house staff member is
signed at the beginning of the term of service and is in effect for the full term of service (1 year).
Renewal of an agreement for an additional term of service is at the discretion of the Residency.
Holidays
Official UAMS holidays are as follows:
Independence Day
Labor Day
Veteran's Day
Thanksgiving Day
Christmas Eve
Christmas Day
New Year's Day
Martin Luther King Day
Presidents’ Day
Memorial Day
UAMS Library
The UAMS Library is housed in the Education II Building and occupies space on three levels. It also
includes the Audio-Visual Library which occupies a part of the fifth floor. The library contains 41,965
books and regularly receives approximately 108 journals related to the behavioral sciences, 4,000
medical journals, and 57 neurology journals. Available databases include MEDLINE, PsycINFO,
CLINICAL MEDICINE, UpToDate, and [email protected]
, among several others.
Mailboxes
Mailboxes are located in TY work room on the 8
th
floor of Shorey.
Resident Room
Each resident will receive a key to the TY Resident Room located on the 8
th
floor or the Shorey Building.
This room is accessible at any time for the TY resident to use for charting, studying or a quiet space.
Name Badges

53
Each house officer will be furnished name badges for UAMS and ACH. It is the responsibility of each
resident to renew badges as they expire during residency. Each house officer will also display a blue
“Resident Physician” hang tag from their name badge.
Parking
UAMS - All members of the house staff are granted parking privileges in 1 parking deck. Your name
badge is activated to operate the parking gate. The Traffic Office contact number is as follows:
501-686-5856.
Arkansas Children's Hospital -- Parking permit stickers can be obtained from ACH Security Office. The
contact number is as follow: 501-364-3474.
Pay Schedules
House staff members are paid monthly. The stipend payment is direct deposited to the resident’s
bank on the last working day of the month. You may access an electronic copy of your “pay stub” on
the Human Resource website. From the menu option on the left side of the Home Page, click on
Employee Self-Serve, follow the “log on” instructions; on the Overview screen, click on “Benefits and
Payment;” on that screen, click on “Payment” and then “Salary Statement.” You may print out your
pay stub if you wish.
Professional Liability Insurance
Each house staff physician is provided professional liability insurance when on official work.
Tuition Discounts
U of A Tuition discounts extend to interns, residents, fellows (both house staff and post-doctoral fellows
in the basic sciences). The fringe benefit also applies to members of the immediate families in the same
manner that it is available to other full-time employees of UAMS.
Social Media
Use of social media (Facebook, Twitter, Instagram, etc.) is at the discretion of each resident. Residents
need to be aware of the implication of social media presence for a physician is different from a student
or other professional. For example, posts about the workday must take special care to avoid breaches in
HIPAA and confidentiality. Posts that do not break confidentiality but that speak pejoratively or
judgmentally about a patient(s), region, or those sharing a diagnosis, reflect poor professional
boundaries and may compromise patient care at a later date if these comments surface when caring for
such an individual. In addition to issues of patient confidentiality, residents should take caution not to
speculate on diagnoses or treatment for individuals portrayed in the news or on social media. Residents
should also be aware that personal disclosures, personal information, and photographs that are posted
in the public domain may be viewed by patients, family members, and future employers. This content
can affect patient care or future hiring opportunities; extremely careful thought and caution should be
given to confidentiality settings on all social media accounts.
Resident Participation in Non-Departmental UAMS Activities/Public Service

54
When engaged in non-remunerative activities in which a resident might be reasonably perceived by
the public to represent UAMS, advance clearance from the Office of the Residency Director is
required.
Educational Fund
The UAMS COM Transitional Year Residency Program encourages residents to practice self-directed
learning using resources outside the formal training program. This includes use of educational materials
and literature and attendance at local and national meetings.
To this effect, each resident is offered a one-time $500 stipend to pay for medical-related books,
educational material or USMLE Step 3 fees.
55
APPENDIX
“Think of yourself as on the threshold of
unparalleled success. A whole, clear, glorious life
lies before you. Achieve! Achieve!”
~Andrew Carnegie

56
My Mistake Curriculum
Transitional Year Residency Program
UAMS College of Medicine
Description of Educational Experience
“My Mistake” is a tool designed to teach and evaluate the Accreditation Council for Graduate Medical Education
(ACGME) core competencies of practice-based learning and improvement (PBLI) and systems-based practice (SBP).
It is important for interns to understand key components of understanding the interaction of their practices within
the larger health system, knowing practice and delivery systems, and being an advocate for patients within the
health care system.
Making mistakes while practicing medicine will always happen, especially at the intern level when young
physicians are making daily decisions about patient care. It is important for new physicians to understand that
mistakes happen, admit their mistakes, realize how mistakes occur, and use the lessons learned to make sure they
and hopefully others do not repeat the same mistake again.
“My Mistake” is a tool that will be used to help Transitional Year (TY) residents understand how their interactions
in the medical system can affect and improve patient care. Examples of common mistakes include: sign out or
transfer errors, order entry errors, and nursing interactions. Fatigue, miscommunication, and knowledge deficits
are a few factors that can lead to errors.
TY residents will be briefed about this assessment tool at the start of the academic year. In the second half of the
academic year, the resident will prepare a presentation outlining one case where a mistake occurred and their
analysis of this mistake. This will be formally presented to fellow TY residents and faculty in one of the Transitional
Year didactic meetings. A copy of this presentation will be placed in the resident’s file and portfolio, and will be
used for quality improvement and patient safety recommendations at the hospital level if applicable.
Overall Goals
• Using the “My Mistake” curriculum, residents are expected to demonstrate an awareness of and
responsiveness to the larger context and system of health care by identifying a mistake that was made and
reflecting on the factors involved.
• Residents are expected to analyze the nature of the mistake and synthesize a rational approach to preventing
similar mistakes from occurring in the future.
Practice- Based Learning and Improvement
Goal
Residents must demonstrate the ability to investigate and evaluate their care of patients, to appraise and
assimilate scientific evidence, and to continuously improve patient care based on constant self-evaluation and
lifelong learning. Residents are expected to develop skills and habits to be able to:
Competencies
• Systematically analyze practice, using quality improvement methods, and implement changes with the
goal of practice improvement.
• Participate in the education of residents and other health professionals.

57
Objectives
• The TY resident will reflect on a mistake that was made during the intern year and determine the factors
involved, as measured by a “My Mistake” portfolio project and evaluation.
• The TY resident will educate other residents about an error that was made by presenting the case to his or
her colleagues in an educational forum, as measured by a “My Mistake” portfolio project and evaluation.
Systems Based Practice
Goal
Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care,
as well as the ability to call effectively on other resources in the system to provide optimal health care. Residents
are expected to:
Competencies
• Advocate for quality patient care and optimal patient care systems.
• Participate in identifying systems errors and in implementing potential systems solutions.
Objectives
• The TY resident will analyze the mistake that was made and the patient or family’s reaction to the mistake
if applicable, as measured by a “My Mistake” portfolio project and evaluation.
• The TY resident will reflect on the mistake, determine if there are potential system errors that could be
improved upon, and give recommendations to implement potential system solutions if applicable, as
measured by a “My Mistake” portfolio project and evaluation.
Professionalism
Goal
Residents must demonstrate a commitment to carrying out professional responsibilities and an adherence to
ethical principles. Residents are expected to demonstrate:
Competencies
• Accountability to patients, society, and the profession
Objectives
• The TY resident will adhere to ethical principles and display a commitment to carrying out professional
responsibilities by taking responsibility and notifying others of the mistake, as measured by a My Mistake
portfolio project and evaluation.
Interpersonal and Communication Skills
Goal
Residents must demonstrate interpersonal and communication skills that result in the effective exchange of
information and teaming with patients, their families, and professional associates. Residents are expected to:
Competencies
• Communicate effectively with physicians, other health professionals, and health related agencies.
• Work effectively as a member of leader of a health care team or other professional group.
Objectives

58
• The TY resident will lead a discussion among his or her peers and discuss the mistake in the format
prescribed and present the topic clearly and logically to the group, as measured by a “My Mistake”
portfolio project and evaluation.
Teaching Methods
1. Self-reflection: The TY resident will use self-reflection to determine the cause of the mistake and potential
solutions to prevent further errors of the same type. To facilitate this educational process, the resident
will use the following format:
• Give a brief description of the circumstances surrounding the mistake.
• What was your specific role in the mistake?
• What factors contributed to the mistake (i.e. fatigue, miscommunication…)?
• What did you do when you realized the mistake was made?
• Did you tell your team and how did they react?
• Did you or someone from your team tell the patient (if a patient was involved)?
• How did the patient or patient’s family react (if a patient was involved)?
• What could be done to prevent others from making this same mistake?
2. Group discussion: The transitional resident will present the case to the program director, staff, and
transitional resident peers during a group didactic session. This will allow for a group discussion on the
factors involved and allow all TY residents to participate in the educational process. The overall teaching
goals for the group discussion are to emphasize the following:
• Realize that everyone makes mistakes.
• Become more comfortable discussing mistakes.
• Improve insight into mistakes and how they happen.
• Contribute to hospital quality outcomes and patient safety through recommendations to prevent
future mistakes from occurring.
Assessment Method (Residents)
• The program director or staff will evaluate the presentation of the mistake using a standard evaluation
form. All interns will evaluate their peers using a standardized evaluation form.
Assessment Method (Program Evaluation)
• Anonymous Resident Feedback: Residents will complete an evaluation of the Transitional Year program at
the end of the academic year. They will provide feedback on the curriculum and outline areas for
improvement.
Level of Supervision
• The educational experience and presentation will be supervised by the program director or staff.
Educational Resources
• Residents should access online references through the use of their issued laptop or hospital computers to
educate themselves about their patient encounters during the rotation. Specific references include: Up-
To-Date, MD Consult, PubMed, OVID, and textbooks and journals available in the medical library. Online
references are available through the medical library site.

59
Transitional Year Residency Program “My Mistake” Questionnaire
UAMS College of Medicine
1. Give a brief description of the circumstances surrounding the mistake.
2. What was your specific role in the mistake?
3. What factors contributed to the mistake (i.e. fatigue, miscommunication…)?
4. What did you do when you realized the mistake was made?
5. Did you tell your team and how did they react?
6. Did you or someone from your team tell the patient (if a patient was involved)?
7. How did the patient or patient’s family react (if a patient was involved)?
8. What could be done to prevent others from making this same mistake?
Address the situation from multiple perspectives – personal, patient, team, service, larger hospital system,
others as are appropriate.
The objective of this is to allow your peers to learn from your mistake but also to identify system issues that
might be targets of future QI/PS projects.

60
Transitional Year Residency Program
UAMS College of Medicine
Resident name: __________________________________________ Date: _________________
My Mistake Topic: ______________________________________
(Check any and all that apply to the topic chosen for discussion.)
Practice Based Learning and Improvement
At level of medical
student
At level of
early intern
At level of
graduating intern
At level of
resident
Milestone PBLI1. Identifies strengths,
deficiencies, and limits in one’s knowledge and
expertise. Sets learning and improvement goals.
Milestone PBLI2. Locates, appraises, and
assimilates evidence from valid sources.
Identifies and performs appropriate learning
activities. Uses information technology to
optimize learning.
Interpersonal and Communication Skills
Milestone ICS1. Communicates effectively with
patients, family, and the public as appropriate
across a broad range of socioeconomic and
cultural backgrounds.
Milestone ICS2. Communicates effectively with
physicians, other health professionals, and health
related agencies.
Systems Based Practice
Milestone SBP2. Works in interdisciplinary teams
to enhance patient safety and improve patient
care quality.
Professionalism
Milestone Prof1. Demonstrates compassion,
integrity, and respect for others, as well as
sensitivity and responsiveness to diverse patient
populations, including to diversity in gender, age,
culture, race, religion, disabilities, and sexual
orientation.
Milestone Prof2. Demonstrates knowledge about,
respect for, and adherence to the ethical
principles relevant to the practice of medicine,
remembering in particular that responsiveness to
patients that supersedes self-interest is an
essential aspect of medical practice.
Milestone Prof3. Demonstrates accountability to
patients, society, and the profession.

61
Comments:
Presentation Effectiveness Criteria
To what extent did the presentation represent the
following features?
Yes
Needs
Work
No Comments
1. Purpose communicated clearly.
2. Organized and easy to follow.
3. Presenter exhibited a good understanding of topic.
4. Presenter was well-prepared.
5. Presenter spoke clearly/effectively
6. Time for presentation used effectively.
7. Slides enhanced presentation.
8. Presenter responded effectively to audience
questions and comments.
9. Presentation was done in a way that engaged
audience.

62
My Reflection Portfolio Project Curriculum
Transitional Year Residency Program
UAMS College of Medicine
Description of Educational Experience
The “My Reflection” portfolio projects are designed as a learning activity to allow Interns to reflect on a specific
event or situation they encountered during a rotation. This project does not require references, only the
Transitional Year (TY) resident’s thoughts, self-reflection, and identification of strengths, weaknesses, and plan for
improvement. TY residents submit their written project to the TY Program Director (one each in December and
May). Feedback is given to the resident and the project is evaluated using the evaluation form. Examples of “My
Reflection” portfolio projects may include discussing an ethical dilemma that was faced and how it was handled,
summarizing a key medical lesson learned during the rotation, or discussing insight that was gained about a
specific aspect of the healthcare system during the rotation.
Overall Goals
• Using the “My Reflection” curriculum, TY residents are expected to demonstrate an ability to analyze their
own practice for needed improvements through self-reflection.
• TY residents are expected to understand the interaction of their practices with the larger system, display
knowledge of practice and delivery systems, and be an advocate for patients within the healthcare system.
• TY residents are expected to gain sensitivity to culture, age, gender, and disability issues through self-
reflection of learning situations that may occur during each rotation.
Teaching Methods
The TY resident will learn through self-reflection of experiences and events encountered during each rotation and
feedback given from rotation supervisors and program faculty. To facilitate this educational process, the TY
resident will use the following format:
• Summarize the case or experience you will reflect upon.
• Briefly describe why you chose this case or situation to reflect upon.
• Self-reflective statement: Identify individual deficiencies or strengths, system deficiencies or
strengths, and/or areas of varied practitioner approaches as they pertain to your case. Devise a plan
for improvement of self or the system if needed. Assess what you learned from this case/experience
and how it will change the way you practice medicine in the future. If applicable, devise a plan for
improvement/future learning.

63
My Reflection Portfolio Project
Transitional Year Residency Program
UAMS College of Medicine
Resident Name: ______________________________
Date: ______________________________
Name of Rotation: ______________________________
Instructions: Biannually, you will reflect upon a specific event or learning point that was unique to the rotation or
healthcare system. This project does not need references, only your thoughts about a situation that you
encountered and learned from. Examples include discussing an ethical dilemma that was faced and how it was
handled, summarizing a key medical lesson learned during the rotation, or discussing insight that was gained about
a specific aspect of the healthcare system during the rotation. You will write your reflection using the format
below. You will give a copy of this completed project to your rotation attending with sufficient advance notice for
its contents to be reviewed and feedback be given before the program deadlines. You and your rotation attending
must sign the bottom of the project. You will give a copy of your write up and signed evaluation to the Program
Coordinator.
1. Summarize the case or experience you will reflect upon.
2. Briefly describe why you chose this case or situation to reflect upon.
3. Self-reflective statement. Identify individual deficiencies or strengths, system deficiencies or strengths,
and/or areas of varied practitioner approaches as they pertain to your case. Devise a plan for improvement
of self or the system if needed. Assess what you learned from this case/experience and how it will change
the way you practice medicine in the future. If applicable, devise a plan for improvement/future learning.

64
My Reflection Evaluation Questions
Transitional Year Residency Program
UAMS College of Medicine
Resident name: __________________________________________ Date: _________________
My Reflection Topic: ______________________________________
(Check any and all that apply to the topic chosen for discussion.)
Practice Based Learning and Improvement
At level of medical
student
At level of
early intern
At level of
graduating intern
At level of
resident
Milestone PBLI1. Identifies strengths,
deficiencies, and limits in one’s knowledge and
expertise. Sets learning and improvement goals.
Interpersonal and Communication Skills
Milestone ICS1. Communicates effectively with
patients, family, and the public as appropriate
across a broad range of socioeconomic and
cultural backgrounds.
Systems Based Practice
Milestone SBP2. Works in interdisciplinary teams
to enhance patient safety and improve patient
care quality.
Professionalism
Milestone Prof1. Demonstrates compassion,
integrity, and respect for others, as well as
sensitivity and responsiveness to diverse patient
populations, including to diversity in gender, age,
culture, race, religion, disabilities, and sexual
orientation.
Milestone Prof2. Demonstrates knowledge
about, respect for, and adherence to the ethical
principles relevant to the practice of medicine,
remembering in particular that responsiveness to
patients that supersedes self-interest is an
essential aspect of medical practice.
Milestone Prof3. Demonstrates accountability to
patients, society, and the profession.
Comments:
______________________________ ____________________________ ____________
Printed name of TY program director Signature of TY program director Date

65
Formal Case Presentation Outline
Transitional Year Residency Program
UAMS College of Medicine
Description of Educational Experience
Purpose: The TY resident will choose an interesting case encountered during a clinical rotation or a
medical question formulated from a patient encountered or discussed during a clinical rotation and
effectively present this case to other TY peers and faculty to provide for an educational discussion
Goal: To effectively present a thorough case presentation and demonstrate that the TY resident is able
to evaluate relevant literature and decide if the literature supports the need to make a clinical change or
manage a case in a different manner.
Expectations: A PowerPoint presentation incorporating all pertinent patient and disease state data. The
presentation should not exceed 35-40 minutes in length to be followed by a 10-15 minute question and
answer session.
Outline
• Introduction
o The main purpose is to place the case in a clinical context and explain the importance or
relevance of the case.
• Case Presentation
o this should be chronological and detail the history, physical findings, investigations,
followed by the patient’s course
History
Physical examination (pertinent positives and negatives; vitals)
Investigations (pertinent lab, radiology, other studies)
Hospital/clinic course
• Discussion
o The main purpose is to articulate the lessons learned from the case. It should describe
how a similar case should/could be approached in the future. It is sometimes
appropriate to provide background information to understand the pathophysiology
mechanisms with the patient’s presentation, findings, investigations, course, or therapy.
Explain why this case was selected.
Does it present a unique challenge or unusual problem—are there other similar
cases in the literature?
Does it illustrate effectiveness of an intervention---does the literature support
this or a need to make a clinical change?
What can other learners/audience add to help in management of this case or
alternative approaches?
• Literature citations

66
Assessment Method (residents)
The program director or staff will evaluate the presentation using a standard evaluation form. All TY
residents will evaluate their peers using a standardized evaluation form.
Level of Supervision
The educational experience and presentation will be supervised by the program director or staff.
Educational Resources
A didactic conference focusing on the “how to’s” of scholarly activity/products, reviewing the literature,
accessing electronic medical literature is scheduled in the first 2 months of the Transitional Year.
Residents should access online references through the use of their issued laptop or hospital computers
to educate themselves about their patient encounters during the rotation. Specific references include:
Up-To-Date, MD Consult, PubMed, OVID, and textbooks and journals available in the medical library.
Online references are available through the medical library site.
67
Sample Case Presentation
Demographics
J.J. is a 37-year-old male with a Spanish surname referred to the program following a positive test for
marijuana at his place of employment. He works on the crew of an oil rig. He currently lives alone after
being kicked out of his apartment by his wife of five years. He has no children from the current
relationship but has a 15-year-old son from his first marriage. He denies any particular religious or
spiritual orientation but acknowledges having been raised in the Catholic Church. He speaks Spanish
and English, and he reports associating primarily with people who speak Spanish.
Key findings
The client denies using marijuana. He says he was at a party where some people were smoking, and
that he must have tested positive because of their use. He acknowledges drinking several beers at
parties like these but denies that alcohol is an issue for him. He says he does not know why his wife
kicked him out other than that “she’s a bitch.” He does not see his son or his first wife. His longest
employment is about two years—on his present job—and he acknowledges having been fired on “a
few” occasions but does not acknowledge why. He says he is willing to complete a CD program just “to
get them off my back,” but insists that he does not have any problems that need attention.
Background
The client was raised primarily by his mother and older sisters after his father left the family when the
client was about four. He did not see his father much after that. He reports average grades in school
until he dropped out in the 10
th
grade to hang out with his friends. He did not finish high school and has
not completed a GED. He has had several jobs, all of which apparently involved manual labor. He
reports “a few” arrests for alcohol related crimes; the most recent was five years ago for DUI. He has
never been in treatment.
Formulation
The client’s ways of thinking are consistent with his culture. Whether or not he actually uses marijuana,
he denies a problem. He may have issues with intimacy related to his father’s abandonment and as
evidenced by his relationship with his son. The pattern of employment and the relationships with his
wives suggest poor interpersonal skills.
Interventions and Plan
I attempted to develop rapport using active listening and reflection. The plan is to continue assessment,
and through motivational interviewing, attempt to identify an area that the client considers a concern.
Allow him to participate in an outpatient CD program to avoid adverse consequences at work, to
enhance the likelihood that he will learn some new social skills, and to give opportunity to form a new
social network.
Reasons for Presentation
Although this case appears routine, I am concerned that I may be overlooking something or that a
different formulation of the case might produce a better chance for a positive outcome.

68
University of Arkansas for Medical Sciences
Transitional Year Residency
Tri-Annual Review (TAR)
Resident Name: _____________________________
Date: _____________________________________
ACGME Requirements
Months
Completed
Milestones
Ambulatory Care
1 month
(140 hrs)
PC1
PBLI1
Emergency Medicine
1 month
(140
hrs)
PC2
PBLI2
IM Wards
2
months
PC3
PBLI3
IM Wards or MICU
1 month
PC4
PROF1
Selective 1: IM Wards, GS,
or Peds Wards
1 month
PC5
PROF2
Selective 2: IM Wards, GS,
EM, Peds Ward, Ped
combined Outpatient
1 month
PC6
PROF3
Total FCS
7
months
PC7
PROF4
Elective:
1 month
MK1
ICS1
Elective:
1 month
MK2
ICS2
Elective:
1 month
SBP 1
ICS3
Elective:
1 month
SBP 2
ICS4
Elective:
1 month
SBP 3
NOTE:
Progress/improvement on core
competencies:
PC = Patient Care; MK = Medical Knowledge; SBP = Systems
Based Practice; PBL = Practice Based Learning; PROF =
Professionalism; ICS = Interpersonal Communication Skills;
Additional Program Requirements
Patient Log completed
monthly
1
st
TAR
2
nd
TAR
3
rd
TAR
Scholarly Work and Other Required Projects
Lecture Attendance
Dates Completed
Work Hours completed
monthly
“My Reflection”
NRMP update/status:
“My Mistake”
Journal Club
Case Presentation

69
Review of Resident’s Self Evaluation: Initial Self Evaluation Mid-year Self Evaluation
1. Review of TY resident’s general goals for TY: -
_____________________________________________________________________________________
_____________________________________________________________________________________
Self-Identified Strengths: -
_____________________________________________________________________________________
_____________________________________________________________________________________
Self-Identified Opportunities for Improvement:
_____________________________________________________________________________________
_____________________________________________________________________________________
New Goals identified:
_____________________________________________________________________________________
2. Performance on Clinical Rotations: Satisfactory Unsatisfactory (circle one)
Concerns or comments:
_____________________________________________________________________________________
_____________________________________________________________________________________
3. Has the TY resident had opportunities to express concerns about the program? Y or N (circle
one)
Comments or concerns:
____________________________________________________________________________________
4. Are there opportunities for assistance on an educational and/or personal level? Y or N (circle
one)
Comments or concerns:
_____________________________________________________________________________________
5. Is the resident functioning at a level commensurate with his or her level of training? Y or N (circle
one)
Remediation/extra assistance required in the following areas:-
_____________________________________________________________________________________
_____________________________________________________________________________________

70
6. Other Issues or comments by the Training Director:
_____________________________________________________________________________________
_____________________________________________________________________________________
7. Other issues or comments by Resident:
_____________________________________________________________________________________
_____________________________________________________________________________________
TY Residency Training Director: ______________________________ Date: _________________

71
UAMS
Graduate Medical Education
Anonymous Evaluation by Transitional Year Resident of Rotation and Attending
Rotation Information
Rotation Name:
Attending Name:
Rotation Month:
Supervising Resident/Fellow:
Instructions:
This evaluation form has been designed to provide a rapid and comprehensive way of evaluating a clinical rotation and
attending supervision. In completing the form, please note the following:
A. All parts are not applicable for all rotations. If a question is not applicable, please indicate so in comments. If there has been
no opportunity to observe the particular activity, please indicate - no information.
B. Please rate the attending in accordance with your expectation for that point in training.
C. We encourage detailed comments, but all ratings of unsatisfactory and needs to improve must have documentation.
A set of written goals and objectives for this rotation was made available to you? □ YES □ NO
Administrative Responsibility
1 = Poor
2 = Fair
3 = Good
4 = Very
Good
5 = Excellent
NA
Attending’s
availability,
promptness in
returning calls.
Attending’s
promptness and
adherence to
schedule.
Attending’s
compliance with
work hours.
Supervising
resident/fellow’s
availability,
promptness in
returning calls.
Supervising
resident/fellow’s
sharing of
workload.
Teaching/Education
1 = Poor
2 = Fair
3 = Good
4 = Very
Good
5 = Excellent
NA
Attending’s
teaching ability.
Comments:

72
Attending’s
ability to engage
house staff in
participation in
a
nonthreatening
manner.
Supervising
resident/fellow’s
teaching ability.
Professionalism/Interpersonal & Communication Skills
1 = Poor
2 = Fair
3 = Good
4 = Very
Good
5 = Excellent
NA
Attending
served as a role
model.
Attending’s
sensitivity and
caring toward
patients and
modeling
patient and
family centered
care.
Attending’s
respect for
house staff.
Supervising
resident/fellow
served as a role
model.
Supervising
resident/fellow’s
equal treatment
of TY resident.
Medical Knowledge
1 = Poor 2 = Fair 3 = Good
4 = Very
Good
5 =
Excellent
NA
Attending’s overall
fund of knowledge.
Attending’s knowledge
of current literature.
Comments:
Comments:

73
Supervising
resident/fellow’s
overall fund of
knowledge.
Patient Care
1 = Poor 2 = Fair 3 = Good
4 = Very
Good
5 =
Excellent
NA
Quality of attending’s
patient care.
Quality of supervising
resident/fellow’s
patient care.
Utilization of evidence-
based medicine in
patient care.
Were you given the
opportunity to assess
patients and develop a
care plan?
Yes
No
Your level of
responsibility for
patient care was…
Too Little
Appropriate
Too High
Practice – Based Learning & Improvement
1 = Poor 2 = Fair 3 = Good
4 = Very
Good
5 =
Excellent
NA
Attending’s
encouragement of
further learning review
of current literature
and growth of TY
resident.
Supervising
resident/fellow’s
encouragement of
further learning review
of current literature,
growth of the TY
resident.
Comments:
Comments:

74
System Based Practice
1 = Poor 2 = Fair 3 = Good
4 = Very
Good
5 =
Excellent
NA
Physician teams focus
on decreasing errors
and improving patient
care.
Comments:
Comments:
The strongest educational learning experiences for this rotation:
Opportunities for improvement in educational learning experiences for this rotation:
75
UAMS
Graduate Medical Education
Transitional Year Didactic Evaluation
Presentation Information
Presentation Title:
Presenter Name:
Date:
This questionnaire gives you the opportunity to provide feedback on various aspects of didactic activities. This
information will be used to guide scheduling of presentations in the future. Please answer all of the questions, if
applicable, and make appropriate comments.
1 = Strongly
Disagree
2 = Disagree
3 = Neutral
4 = Agree
5 = Strongly
Agree
NA
This presentation
provided material
beneficial to you.
(applied to patient
care)
This presentation
was appropriate
to your education
level.
The material was
presented in a
stimulating
manner.
This presentation
should be given
to future
residents.
The material
should be given
to future
residents by the
same presenter.
The presenter
was
knowledgeable
about the subject
material.
Questions were
allowed and
answered
appropriately.
An appropriate
amount of time
was provided for
the topic.
Handout
materials were
helpful.

76
Comments:

77
Transitional Year Resident
Final Summative Evaluation
Re: [TY Resident Name]
PGY-1, Transitional Year Resident
[date]
Dr. [name] entered the UAMS Transitional Year Residency training program on [date] and has
satisfactorily complete his/her training effective [date]. (S)he graduates training in [good] academic
standing and at the time of this report is able to function at the level commensurate with completing
one year of post-graduate training. Dr. [name] has completed all clinical rotations satisfactorily and has
met the requirements of 28 weeks of fundamental clinical skill areas including 140 hours of emergency
medicine and 140 hours of ambulatory care experience. (S)he has demonstrated progressive
improvement of competency, appropriate to his/her educational level, in all of the six GME identified
core competency areas. At all times during his/her one year of post-graduate training the Transitional
Year residency, Dr. [name] has evidenced professional behavior and clinical competence.
Dr. [name] completed all core rotations and elective rotations in a very solid fashion. Faculty members
rated Dr. [name] [describe general ratings in clinical rotations]. Dr. [name] actively participated in
didactic/seminars throughout his/her Transitional Year training. During his/her clinical rotations and
seminars, it was evident that Dr. [name] made progress in his/her skills and knowledge. As such, Dr.
[name] participated in a process of graduated supervision commensurate with his/her level of training.
Dr. [name] also had an opportunity to evaluate teaching faculty, didactic instruction, and the overall
program during the Transitional Year. Dr. [name] completed documentation requirements in a timely
manner throughout his/her training. (S)he was not the subject of any disciplinary or malpractice actions
during his/her Transitional Year residency training.
Dr. [name] participated in scholarly activities during the Transitional Year residency program including
[list here]. (S)he actively participated in the Transitional Year journal club and in a quality improvement
project, [list here], and successfully completed Institute for Healthcare Improvement (IHI) Open School
online courses including improvement capability; patient safety; triple aim for populations; person-and
family-centered care; leadership; and quality, cost and value.
Dr. [name] has/has not successfully passed USMLE Step 3. Post-graduation from our program, Dr.
[name] will be entering a categorical residency in [specialty name] at [training site name].
Jason S. Mizell MD FACS FASCRS
Program Director, Transitional Year Residency
Professor of Surgery
Director of Business of Medicine
UAMS College of Medicine
